

There are three lead systems that make up the standard ECG:
- Standard Limb Leads (Bipolar): I, IlI & III
- Augmented Limb Leads (Unipolar): aVR, aVL & aVF
- Precordial Leads: V1- V6
The Standard Limb Leads are used to display a graph of the potential difference recorded between two limbs at a time, ergo, they are bipolar. In these leads, one limb carries a positive electrode and the other limb, a negative one.
The three limb electrodes, I, II and III form a triangle (Einthoven’s Equilateral Triangle), at the right arm (RA), left arm (LA) and left leg (LL).
The three Standard Limb Leads:


Einthoven’s Law explains that Lead II’s complex is equal to the sum of the corresponding complexes in Leads I and III and is given as II = I + III
For example,
- If you had an ECG in which the Lead I R wave was 7mm tall and the S wave 2mm tall, subtract the S from the R, and you would have 5mm.
- On the corresponding complex in Lead III, the R wave measures 1mm and the S has a negative deflection of 16mm. Subtracting the R from the S gives -15mm
- In Lead II, using the same method as before, you get a measurement of -10mm
Using these measurements with Einthoven’s Law you get
- II = 5 + -15 = -10
So these leads are electrically equilateral.
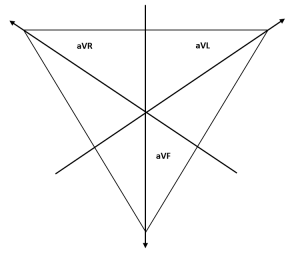
The Augmented Limb Leads obtain a graph of the electrical forces as recorded from one limb at a time using a null point with a relative zero potential, thus, they are unipolar.
These leads, aVR, aVL and aVF give additional views on a trace by reading potential difference across the heart in three more directions on the frontal plane.
The three Augmented Limb Leads:


The Right Leg (RL) electrode removes artefact from the ECG and is not a directly participating factor in the visible trace.
The Precordial Leads, or Chest Leads are labelled V1- V6 and are placed on the sternum travelling in a posterior direction:

- V1
- Fourth intercostal space, on the right sternal border
- V2
- Opposite V1, on the left sternal border
- V3
- Between V2 and V4
- V4
- Fifth intercostal space, on the mid-clavicular line
- V5
- Same level as V4, anterior axillary line
- V6
- Same level as V4, mid-axillary line
This direction creates a transverse plane via which to view the heart’s electrical signal, in addition to the frontal plane offered by the Limb Leads.
Lead Groupings or Contiguous Leads are categories of leads based on the area of the heart they examine:
- Inferior
- “Look” down, towards the feet
- Leads II, III, aVF
- Antero-septal
- Overview the ventricular septum and anterior wall
- Leads V1, V2
- Anterior
- Predominantly over anterior wall
- Leads V3, V4
- Lateral
- Examine lateral wall
- Leads V5, V6
- Leads I, aVL (High Lateral)
Polarisation dictates the direction of the trace on the ECG.
- A wave of polarisation travelling toward a positive electrode results in a positive deflection on the ECG.
- A wave of polarisation travelling away from a positive electrode results in a negative deflection on the trace.
- A wave of depolarisation travelling at a right angle to a positive electrode results in a biphasic deflection on the trace.
To graphically represent the electrical forces in Einthoven’s Triangle, we can draw them in such a way that they bisect each other, passing through a common central point.

Each axis is separated by 60° from each other, with the lead polarity , + or -, remaining in the same direction. This is known as the Triaxial Reference System.
By combining this triaxial lead system with one from the Unipolar Limb leads (also with 60° separation), we create the Hexaxial Reference System, used to determine the electrical axis of the heart.
ADDED TO:
WHICH CREATES:

Don’t worry about the colours yet. They will become clear when we determine the cardiac axis.
Ref:
Luthra, A. (2007) ECG Made Easy. Third edition. Tunbridge Wells: Anshan
Houghton, A. Gary, D.(1997) Making Sense of the ECG Fifth edition. London: Arnold


Good
LikeLike
Hey this was really helpful 🙂 Thanks!
LikeLike
No problem! If there’s anything you think could be included anywhere on the site, let me know! 😊
LikeLike
Will do 😊your piece was helpful for an assignment for my instrumentation course. Are you a med student?
LikeLiked by 1 person
No, I’m a Clinical Physiologist (qualified 7 weeks ago); I perform and interpret the diagnostics that you guys use to create a treatment pathway. Pacemakers, ECG, Echocardiography and angiograms.
LikeLike
I have found the precordial leads to be labeled as “V” standing for Voltage and Vector. Which one is correct when referring only to V1-V6?
LikeLike
I’ve only ever known them to be known as “vector” if I’m honest (precordial vector 1, 2, 3… etc). I appreciate this is far from a definitive answer, though, and as such I’m happy to be corrected!
LikeLike
Very helpful, thank you.
LikeLiked by 1 person
Why is Lead II used as a typical ECG? Thanks.
LikeLike
Lead II displays the activity closest to the actual cardiac axis, so it gives the most accurate depiction of true P and R waves! 🙂
LikeLike