

Acute Coronary Syndrome
Myocardial ischaemia as a result of MI, either non-ST elevated, or ST elevated (NSTEMI or STEMI) or unstable angina
Pathophysiology
The atherosclerotic process within blood vessels creates a vulnerable plaque, which houses a necrosis containing ’tissue factor’. When the plaque becomes disrupted and tissue factor is exposed to the bloodstream, a coagulation cascade is activated, leading to endothelial vasoconstriction. This, in turn, forms an intraluminary thrombus in the vessel and this occlusion is what gives the endpoint ACS.
Angina
Caused by atherosclerosis of the coronary arteries, restricting the flow of O2 to the cardiac muscle. This leads to a sometimes debilitating pain or a sensation of squeezing in the chest. This pain can also occur in the neck, arms, jaw and back.
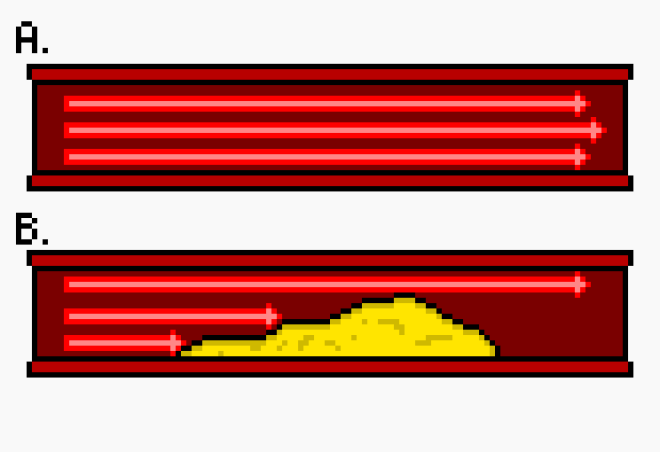
This diagram shows a normal artery with unimpeded blood flow (A) and the plaque build up within the artery, causing it to narrow and restrict the blood flow (B).
- Unstable Angina
- Angina at rest, post revascularisation angina, new onset exceptional angina (less than 2 months old) or a recent acceleration of pervious angina (again, less than 2 months old)
- Stable Angina
- Episodic angina during periods of exercise that are constant over time.
The Canadian Cardiovascular Association uses this classification chart for angina. It is generally accepted worldwide.

Unstable angina is suspected if:
- Pain occurs at rest with a duration of 20+ minutes within one week of index incident
- If previously diagnosed angina develops resistance to medication that controlled symptoms
Rosen’s Emergency Medicine uses these additional guidelines:

Note:
- New onset angina is an automatic Class II classification when the onset is within the previous two months of diagnosis
- Any worsening of chest pain, i.e. an increase in frequency or duration should evoke a +1 class increase
Diagnosable with a rise and fall in serum cardiac biomarkers (troponin), in addition to at least one of the following findings:
- Ischaemic chest pain lasting more than 20 minutes
- ST changes or pathological Q waves in patient’s ECG
- Coronary intervention
- NSTEMI
- Symptoms of unstable angina coupled with positive cardiac biomarkers findings
- STEMI
- Symptoms of unstable angina, positive cardiac biomarkers and ST elevation on ECG
Unstable angina and NSTEMI are incredibly difficult to distinguish from one another upon index admission in that changes in troponin levels are sometimes not detectable for up to 12 hours after onset symptoms.
Dx
Diagnosis of ACS is based on:
- A thorough patient history:
- Character of pain, location and radiation
- Onset and subsequent duration
- Factors which influence aggravation/relief
- Risk Factors:
- Familial Hx
- Smoker status
- Age (55+ is considered a risk factor)
- Hyperlipidemia
- Known Coronary Artery Disease
- A physical examination
- ECG
- Biomarker analysis
Patients can then be divided into several groups:
- Stable angina
- Unstable angina
- Myocardial infarction
- Non-cardiac chest pain
- e.g. gastrointestinal, pulmonary embolus, musculoskeletal
- Cardiac (other)
- e.g. pericarditis, aortic dissection
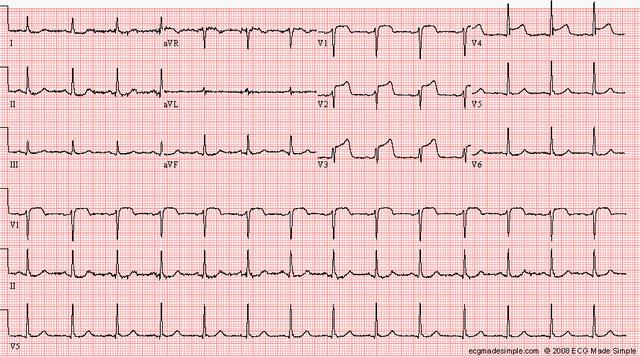
ECG in ACS Dx
The ECG presents great benefit, in that is a quick, non-invasive tool that can guide treatment decisions and also identify causes of symptoms that may differ from those expected.
However, it isn’t a tool with which we can have 100% confidence and a normal ECG does not exclude the presence of ACS. In addition, approximately 50% of patients with acute myocardial infarct display diagnostic abnormalities on their ECG.
Reference:
Zimetbaum, P. New England Journal of Medicine. 2003;34:348:933-40


One thought on “Acute Coronary Syndromes”