

Atrial fibrillation (AF) is the most common non-sinus tachycardia
Typically, AF is caused by rapidly firing foci. Usually, the primary signal would emanate from the sinus node, and then spread across both atria in a controlled manner, before reaching the atrioventricular node, as normal.
In the case of atrial fibrillation, the firing of disorganised impulses originating in the atria and pulmonary veins. This essentially makes the left and right atria ‘quiver’, rather than depolarise and contract in the normal fashion.

This fibrillation does not allow the atria to empty as normal, and thus the blood within them may coagulate, potentially leading to stroke, pulmonary embolism and transient ischaemic attack.
Symptoms associated with atrial fibrillation are diverse, with palpitation being the most usual. Dyspnoea and presyncope (light-headedness and feeling as if about to faint, as oppose to actually fainting), are also common symptoms. Syncope, i.e. actually fainting, and chest pain are less common.
Risk Factors
- The risk of AF increases with age:
- 40-50 years old:
- <0.5%
- ≥80 years old:
- 5-15%
- 40-50 years old:
- It is often undiagnosed, due the need for symptoms to be present upon examination
- Obesity increases risk
- AF also increases the risk of further AF
- Ethnicity
- Stress/ Anger
- Genetic influence
Atrial Fibrillation ECG
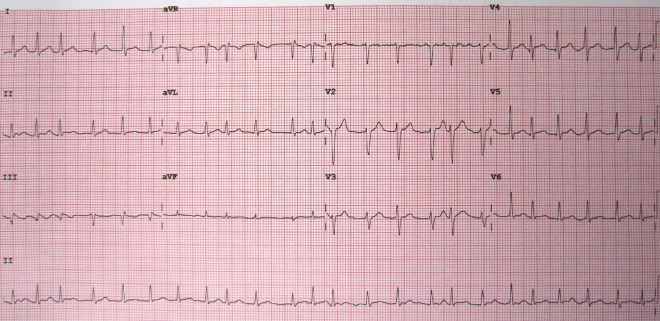
- HR
- >100bpm
- Rhythm
- Irregularly irregular
- Atrial rate can reach 300bpm
- Ventricular rate depends on AV node conduction
- No P waves
- Lack of isoelectric baseline
- QRS complexes:
- <120ms
- Unless there is an existing BBB
- <120ms
- Calculating HR can be done by multiplying the number of RR intervals on 10 second rhythm strip by six, when recorded at 25mm/s.
Atrial Fibrillation Treatment and Classification
When classifying atrial fibrillation in an individual, the point from which one should begin is the detected index event, symptomatic or otherwise. The American Heart Association recommend an approach that categorises in to one of the following:
- Paroxysmal atrial fibrillation
- Episodic AF that spontaneously terminates within seven days, with the majority of episodes lasting no more than twenty four hours.
- Persistent atrial fibrillation
- Episodic AF that lasts over seven days. May require electrical or pharmacologic intervention to rectify
- Permanent atrial fibrillation
- Persistent AF lasting more than one year, either because intervention has failed, or has not been attempted.
The NICE pathway for assessing AF begins with palpation for irregular pulse in patients presenting with the aforementioned symptoms, then further investigation with electrocardiography, both 12-lead and ambulatory, and echocardiography, particularly with those for whom cardioversion therapy is a consideration.
Treatment for AF potentially has three goals; to re-establish and uphold sinus rhythm, to prevent thromboembolism and to control ventricular rate during atrial fibrillation.
Intervention, in the case of AF- cardioversion, can use either pharmacological agents such as ibutilide to alter the electrical properties of the organ itself, thus muting the abnormal rhythms, or electrical direct current to slow the heart rate, which can be repeated.
Ref:
Topol, E., Califf, R., Prystowsky, E., Thomas, J., Thompson., (2007) Textbook of Cardiovascular Medicine. 3rd Ed. Philedelphia: Lippincott Williams and Wilkins
lifeinthefastlane.com

