In amongst busy shifts, I’ve been tweeting about HCS Week 2018, and chatting to other scientists about their experiences. Yesterday, I tweeted a picture of Helen, a specialist Echocardiographer, whilst she was hard at work analysing pulse wave data, and today I’m sharing the answers she gave to a couple of questions I asked her about what she remembers about the history of her job in her 30 years of experience, and her feelings on the changes she’s seen over the years.
With 30 years under your belt, you must have noticed changes in your profession. What’s different now, compared with when you started?
Firstly, my job title has changed. I was a “Cardiac Technician” and began as a student working in Cardio-Respiratory, with a full-time, guaranteed job at the end of my training. I studied on a day-release basis for an ONC then HNC, eventually topping up to BSc when this became compulsory.
Technology has had a big impact on advancement of procedures, which is better for patient quality of life, etc; Cardiac Techs performed all the ECG’s in the hospital, carrying a crash bleep for A&E, and now, of course, there is provision for ECG’s on every ward and dept.
Procedures such as angioplasty and bi-vent pacemakers were not as widely available, either; most CAD patients went on to undergo CABG and only relatively basic bradycardia devices were on offer. Obviously this is all change now.
Alongside this, we are now much busier than ever before and our roles have changed massively. We now carry out duties which years ago only consultants could do. I think this is good for everyone but does mean we have much more responsibility, in addition to greater autonomy. We are, however, still part of a team, which is vital to remember.
Did you have any reservations about the changing nature of your specialism?
I used to worry that becoming more busy and more academic would threaten our profession, that less qualified staff would have to take on more of our roles. Fortunately, routes into this career seem to be more widely available and thus, accessible. Emphasis seems to be more about finding the right person for the job, and training is focused, usually by specialist Scientists who understand the needs of both the students and patients.
It’s important to realise that anyone can be shown how to perform an ECG or assist in a cath lab, but qualities such as initiative, kindness and compassion are inherent traits which cannot be taught, and are absolutely vital in this profession.
It’s been a little while since I’ve posted to the blog, but Healthcare Science week seems like as good a time as any to do pick it up again. I’ll try my best to upload here or to Twitter, each day, be it information on what might be happening up and down the country, or things going on within my own Trust. I’ve also roped some colleagues into answering a couple of questions, too.
HCS week is an annual event celebrating all 85 specialisms within the discipline. As the oft-overlooked scientists within the NHS, it falls to us to put ourselves out there, and this week is the time to do it! Biomedical Scientists, Physiologists (there are a few different types of this particular scientist), Audiologists, Vascular Scientists, and many, many more are showcasing what they do for patients they treat in the NHS, and using the hashtags #HCSWeek18, and #HCSWeek2018, they’re getting it to the masses. We need to inspire the next generation of scientists to join our ranks, so HCSWeek gives us the perfect opportunity to show students and potential scientists exactly how far-reaching their options are.
Today, I spoke to my colleague Oli, who like me, is a newly-qualified Physiologist, about why he opted to undertake a career as a Physiological Scientist, and what he plans on doing, moving forward.
Clinical Physiologist, Oli. Here, he is setting up an exercise tolerance test in an attempt to induce ECG changes associated with angina, and ischemia
What attracted you to this particular scientific career in the first place?
It’s as simple as being able to help people, really. Clinical Physiology allows for patient-facing tests to be performed, so I felt like it would let me make an immediate difference.
Now that you’re qualified, and are well-versed in the basics of the job, are there aspects that you appreciate more from a post-graduate perspective?
Definitely. Every day presents a different challenge, because every patient is different. In the RUH, we have a wide array of clinical skills we have to learn, and as a result, I find that I’m adding to my knowledge every day.
Where do you see your career heading, moving forward?
I’m hoping to specialise in Cardiac Imaging, and have applied to the STP programme to help with that speciality. There are a wealth of options, even after that, so whilst I’m not entirely sure at this stage, I may look at the Higher Specialist Training after that!
Myself and some of my colleagues recently relinquished a Saturday off, and braved the icy cold (read: British) weather to try to meet with the public, and raise awareness of atrial fibrillation through a project spearheaded by the AF Association.
I didn’t organise the event, but was kindly invited along, and jumped at the chance to help some of my amazing Cardiology workmates by checking pulses, and recording rhythm strips using the AliveCor mobile ECG monitor (which I have previously reviewed here).
AF is an atrial arrhythmia, wherein the sinus node does not cause appropriate, rhythmic depolarisation as it normally would. Rather, multiple foci activate, facilitating a motion akin to ‘quivering’, which raises the risk of embolism through the inefficient pushing of the blood into the ventricles. It’s an incredibly dangerous problem if left untreated, so it’s vital that it gets detected, and preferably this would happen early.
I go into detail about AF, it’s mechanisms and ECG presentation in this study guide, so have a look at that if you want to understand it further.
As you may or may not be aware, atrial fibrillation is, globally, the most common clinically significant cardiac arrhythmia, and it is thought that whilst 1.2 million people (a conservative estimate) in the UK are known sufferers of the sinus node disorder, a 500,000 have it, and live undiagnosed. The estimated cost of AF to the NHS was somewhere in region of £2.2 billion, in 2008, and given that the prevalence of the arrhythmia has increased year on year, this number may well be higher now.
Obviously, this is far from an exhaustive exploration of AF, but hopefully it gives some insight into why it’s so important to detect and treat, and why initiatives such as this one are a good idea.
We set up shop in Frome’s Westaway shopping centre at around 10am, where members of the public who’d read about the event in the local newspaper were already queueing. We four clinical scientists proceeded to advise and check 85 people throughout the day. We had a surprise visit from Cardiologist’s Kitchen, too!
Mary, of Cardiologist’s Kitchen fame, showed up to say hello!
Many people we talked to had little-to-no idea what the condition was, its risks, or how it was treated, so we used literature, ECG examples, and a scale model of a heart, to educate, and taught people how to check their own pulse before performing quick rhythm recordings which we analysed on the spot. More than a few people who attended had known AF, and their questions largely involved their current treatment, and the potential impact AF might have on their life. Most, however, visited so they could get checked over, hopefully putting their mind at rest, and learning something in the process.
We didn’t find any new atrial fibrillation (although we did discover two cases of previously undiscovered AV Block), but of equal importance to arrhythmia discovery, was the community engagement, particularly in a public setting. In clinics it’s easy to fall into a cycle with patients, due to schedules and time pressures, and whilst we all try our hardest to make sure everyone is treated individually, seeing the problem before the person is always possible. Interacting with patients on “their turf” meant the ball was in their court, if you like, and the sheer volume of people who expressed an interest meant it couldn’t have been further from a wasted day.
The feedback we received was overwhelmingly positive, and there was a recurring theme in the gratitude people felt for the healthcare environment coming to them, as oppose to the other way around. Many of those to whom we chatted understand the strain that hospitals and GP surgeries are under, and felt that visiting to be checked for AF, and other such things, would be inappropriate. In many ways, I suppose they’re right, too; regardless of the importance of finding these things, especially as they do not always present with obvious symptoms, healthcare centres, unfortunately, cannot cope with the demand a service such as this would present. To this end, I was glad to have ventured out to participate in this, an outdoor clinic of sorts, and educate the public on what to look for, as well as how they can guage their own heart rhythm and take some more control over their own health. I sincerely hope to do it again soon!
The AFA is a fantastic charity, so it’d be great if you were to find out a bit more about them by visiting them here.
I’d like to thank my colleagues for asking me to participate, and generally being fantastic people, those who visited us and asked lots of challenging questions, and the kind souls who bought us ginger ale and flapjacks when the temperature reached what *felt* like sub-zero levels.
The statistics used in this post are taken from the BHF. If you want to take a look for yourself, visit the British Heart Foundation, here.
When Cardiologist’s Kitchen put forward its Health Foundation application, it stated that it would run patient workshops at Neston Park Farm & Kitchen to engage patients with professionals and good, healthy food.
Neston head chef Steve Mercer cooked a fabulous 2-course meal for guests, and after a brief interlude by Ali Khavandi and Mary Fifield, there were some indroductions for myself, nurses in Cardiac Rehabilitation and the CardioFITr team (more on these guys in the future), as well as local food producers Fussels, and Fresh Range, whose ingredients made up some of the food.
The workshop wasn’t about us, however; it was a patient-centred event, so the real stars of the evening came in the form of the service users themselves. A select few were gracious enough to share their stories regarding the improvements that Cardiologist’s Kitchen had made to their lives. One had lost a considerable amount of weight and thus, could do normal, everyday things that she had previously found difficult as a result of her (now greatly improved) angina, another was part of the CardioFITr programme, which, run by healthcare professionals and in conjunction with Cardiologist’s Kitchen, uses evidence-based science and medicine to improve physical fitness and promote a continued change in lifestyle. He too, had seen a considerable and positive reduction in weight and blood pressure, and was almost ready to cease his medication for the latter. This is a particularly palpable achievement for the scheme, and proves it actually supports patients to persevere.
A 2010 paper by Curtis Triplitt of The University of Texas titled Improving Treatment Success Rates for Type 2 Diabetes cites clinical inertia as the biggest barrier to treating the condition, so by beginning to see positive results in this manner, initiatives like this really do matter with regards to health and wellbeing. It’s long been known that diet and exercise have a massive impact on health, but anyone who’s struggled with dieting, knows that support is one of the most important factors in sticking to whatever regime one is using to better their health.
As I chatted to patients and heard their stories, I became aware of just how thankful they were for Cardiologist’s Kitchen, and the positive impact it was having on their lives. Many of them had been rushed to the Catheterization Laboratory with a suspected infarct, and regardless of the findings had assumed their lives were irrevocably altered. The advice and specific support given by CardioKit meant they were now turning a corner and seeing measurable changes in their own health. The best part was knowing that they had essentially been encouraged to do it themselves with their own willpower.
Barely a month goes by without a national newspaper displaying words like “science says _________ is bad for your health”.
Don’t get me started…
I concede that *some* of these headlines might be correct, but it’s worth taking them with a pinch of salt, if you’ll pardon the pun; firstly, “science” isn’t an all-powerful being that performs every possible study single-handedly, so it’s difficult to know exactly who has put forth the particular claim and how many people through whom the information has passed before it gets to the news media, and secondly, “science says…” doesn’t necessarily mean it’s double-blind, peer-reviewed, evidence-based or ethically funded, so between the debunked results of Andrew Wakefield’s infamous autism/ MMR study and big pharmaceutical companies potentially protecting their interests by omitting unfavourable study data, it isn’t a great idea to believe that eating bacon causes your lips to fall off, simply because the junior science editor for The Daily Expresstells you it does.
What, then, do you believe? Nobody wants to find themselves being brought into a Cath Lab, and they don’t want the uncertainty that comes with not knowing whether the food that they’re eating is going to help put them in that position. This is where Cardiologist’s Kitchen comes in; Consultant Interventional Cardiologist Ali Khavandi would rather intervene well before you’re being consented for an invasive procedure, and addresses issues with cholesterol, weight, blood pressure and diet by way of a pre-emptive strike using evidence-based dietary and lifestyle changes.
Cooking Cardiologist, Ali Khavandi
Not unlike this site, the initiative began as a humble health-based blog in 2015, featuring advice and recipes, and was borne through personal, clinical experience. Khavandi’s passion for both cardiology and cooking pushed him to create a resource, and seek a wider market using the same mechanisms employed by the media and the food industry, but using an evidenced basis in cardiovascular wellbeing. The Health Foundation has since granted the Cardiologist’s Kitchen project an award that has allowed the trial of this innovative approach to healthcare to really take off!
Currently, Cardiologist’s Kitchen has partners in GP surgeries, a restaurant and various South West England food suppliers that combine to make conduit for the project’s entire message. Despite still being in relative infancy, Cardiologist’s Kitchen has made headway, and continues to open up avenues via which to get the message out there.
Patients with new or existing high blood pressure can get a CardioKit pack at affiliated GPs. I got one to sample, which contained some money off vouchers, health advice and information about the project. In addition, The Bunch of Grapes gastropub, found in Bradford on Avon, just outside Bath, offers some menu heart-healthy menu items devised by both Ali Khavandi and head chef Steve Carss (I’ve sampled some of these too; they’re delicious).
The recipe for this Chinese chicken and more, is available on the Cardiologist’s Kitchen website
The website is the real central feature of the initiative, with healthy recipes, incentives for transforming your attitude to heart health, and evidence-based discussion on food fact, cutting through scaremongering in the bad science which can sometimes surround food.
Rather marvellously, it encourages the use of local suppliers by offering deals and home delivery on their seasonal produce. They’re also in the process of developing ready meals specifically designed to improve cardiovascular health.
By using CardioKit, the aim is to lessen the need for medication, and support local business as well as your own heart. If you’re reading this, and it applies to you as a patient, then I urge you to have a look. If you’re a practitioner, definitely do the same, and get in contact with the CardioKit team to see how you can get involved.
Inspired by the advice presented on Cardiologist’s Kitchen, I made a rather lovely Jamaican beef curry, the (really easy) recipe for which I will share here:
250g lean diced beef
4 banana shallots, thinly sliced
1 x jalapeno chili, diced. (Leave the seeds in if you’re a daredevil)
1 x carrot, peeled and chopped
1 x small sweet potato, peeled and diced
1/2 mango, diced
2 garlic cloves, sliced
1 box passata
1 tbsp. jerk paste (jerk seasoning will do fine, but add 2 tbsp.)
1tbsp garlic granules
1 tsp. tomato puree
100ml chicken stock
Greek yoghurt
Flat leaf parsley, roughly chopped
Salt and Pepper, to taste
Rice, any kind, and enough to feed 2 people
With a little oil, brown the beef until sealed sufficiently. Add the shallots, sweet potato, and sliced garlic, and cook for another few minutes. Throw in all of the other ingredients and reduce heat. Simmer for 60 mins, or until the beef is tender, and use this time to cook your rice. Serve with some chopped parsley and a dollop of yoghurt.
I recently spent the day inside the catheterisation laboratory, specifically in the pacing lab. After a few relatively straightforward implants, we reached the final case of the day; a pacemaker change. The patient in question had 4 months of reported battery life left on his pulse generator, so on paper, it was merely a case of opening the pocket in which his old device was housed, and switching it out for a new one that would stimulate his heart for the years to come.
Textbooks are great, in that they detail a procedure from start to finish, usually from everyone’s perspective, covering all bases regarding technique, equipment, potential emergencies, and possible troubleshooting options should the need arise.
These emergencies range from device malfunction to cardiac complications, and cover most things in between. I haven’t read a textbook that outlines what should be done if the patient suffers from dementia, however…
The procedure began late due to the difficulty in cannulating the individual, given they didn’t really understand where they were, and began thrashing around wildly in confusion as soon as the needle was introduced, but eventually they were brought into the lab and set up on the table. Local anaesthetic was administered whilst myself and other members of staff present tried to ensure that the patient was as calm as possible.
This proved rather difficult, as the patient was understandably scared; bright lights and masked strangers staring down at you aren’t a pleasant experience for anyone, so add a severe perception deficiency into the mix, and it’s only going to be worse.
Once the procedure proper had begun, it got so much worse.
If you’ve ever been in a lab or theatre when an electrocautery is being used, you’ll know how loud it is. Trying to keep a confused patient calm, and focussed on your voice alone, is incredibly difficult when you’re being drowned out by a deafening beeping noise. The consultant performing the change was having to work 3 times harder than normal whilst completing his task, because of the patient’s inability to understand what was happening, and more importantly, why it was happening.
There were 6 staff in the operating lab, and of those six, the only one able to fully focus on their job was the consultant. The rest of us tried to hold a limb each, to stop them from flailing and causing potential injury.
The chief priority was the patient’s overall well being, so when the radiographer received a rather nasty set of deep scratches, she endured the pain and tried to reassure the patient.
When the registrar’s fingers were being held so tightly together that they almost broke, she quietly asked if I could free them using one of my available hands, and continued talking to the patient.
When I was struck in the face as a result of removing a hand from the patient’s leg in order to do the above, I didn’t make a sound, as I didn’t want to frighten the patient anymore.
In this patient’s mind, we were causing discomfort for no reason, and as a result, this patient was fighting as though his life depended on it, but nobody said anything that might give cause to further agitate him no matter how much was thrown at them in that situation, because the fact is, we were there to help the patient and their safety came before our own.
No amount of reading could have prepared me for that situation, but even a small amount of warning, or advice, would have been a boon. To that end, I’ll say this;
Scenarios such as the above WILL happen. It’s inevitable. Just stay calm, communicate with everyone around you and never forget why you’re there. Of course it’s not right that you sustain an injury on the job, but the bigger picture comes first and then you can set about producing system changes.
Beyond Verbal, an Israeli company leading the market in voice/emotion analysis software are making headlines thanks to their study with the Mayo Clinic, that shows that voice analysis can indicate the presence of coronary artery disease (CAD).
CAD is responsible for one of the highest cardiovascular mortality rates in developed countries globally, and whilst lower in developing countries, this figure is quickly rising. With this in mind, inexpensive, low-risk and non-invasive screening methods are a very desirable prospect. Currently, ECG, Exercise Tolerance Testing (ETT), Radionuclide testing and Pharmaceutical Stress Testing are the most common procedures used to screen for CAD, but, aside from ECG, each has contraindications, and/or is fairly invasive. Again, aside really from a simple ECG, each has a middling to significant associated cost attached to it. Technology that could reduce these costs and the potential for unnecessary testing presents a possible alternative to patients being referred to chest pain clinics and such, without a sure fire reason to do so.
Beyond Verbal have already used their vocal analysis software to find audio characteristics associated with Parkinson’s disease and autism, and have now turned their technology to CAD.
The Beyond Verbal/ Mayo Clinic study hypothesised, due to the association coronary atherosclerosis has with other systemic pathologies, that vocal processes and the structures responsible may also be affected.
150 patients, 120 of which presented for angiography of the coronary arteries and 50 healthy, or non-cardiac control patients had their voice recorded prior to the test. Beyond Verbal then used a variety of their analytical software to record three 30 second voice clips from each patient; the first (R1) was a predetermined script, R2 was a description of a positive experience, and R3 was personal like R2, only a negative experience.
The analysed results show a 19-fold increase in the likelihood of CAD in R3, the negative voice clip, irrespective of traditional cardiac risk factors such as age, suggesting there is indeed a link between CAD and voice.
BV hope that future development of this technology can be used to screen patients telephonically.
On the 10th of November, after a long process of meetings between local council members, healthcare union staff and members of the public, Bath and North East Somerset council voted in favour of Virgin Care for its delivery of adult services in the area, rejecting the rival bid from ousted former controllers, Sirona CIC.
B&NES council have given their reasons for preferring Virgin Care for this role, citing their transforming services across the country and positive collaboration with GPs, care centres and charities as two of those at the forefront of the decision.
It is important to note that B&NES has made this decision with deep input from the local Clinical Commissioning Group and community champions over two years, so it is the culmination of a number of differing viewing perspectives and backgrounds.
The vote, which was 35/22 in favour of the Richard Branson-owned healthcare firm, marks the first time a for-profit organisation has been in charge of NHS contracts in the B&NES area. It has been met with vehement opposition from numerous individuals and local organisations since the bid was announced, and the company itself has previously been under scrutiny for its use of tax havens, quality of care, and alleged mistreatment of staff.
National outlets have lambasted VC in the not too distant past
In 2012, a Dispatches documentary revealed how under-target a Virgin Care centre was regarding Chlamydia screening, exposed a memo asking staff to take test kits home with them, in order to increase the number of screens executed and keep them in line with national targets.
A year later, emergency department medics and the CQC expressed deep concern with practice policy, after a VC-run centre triaged a patient using a receptionist as oppose to a healthcare professional. This proved fatal, but Virgin still defended their actions at a hearing, saying that the patient was appropriately treated.
Despite only being in the market since 2010, Virgin Care currently has NHS contracts worth a reported £1bn, and provides services across the country. It being a Virgin subsidiary and having its head offices in the British Virgin Islands, means it is exempt from corporation tax, but, tax aside, the company has said that all profits made by its B&NES services are to be re-invested into local healthcare delivery. At the same time, however, it has been made clear by the company itself and from other sources that Virgin Care are not looking to make profit from this deal.
Confused yet? I am.
With this deal citing a new precedent in the volume of healthcare services of which Virgin Care have control in the UK, confusion isn’t something that benefits patients, and the majority of middling to major news networks have sensationalised this to the point of farce;
The Canary used the headline “While We’re Still Recoiling from Trump, Branson Quietly Buys up the Biggest Chunk of our NHS…”
Given that this deal has been featured in local and national news for well over a year, spawned public and political backlash (acclaim too, in fairness), and has only now reached a conclusion, the word “quiet” isn’t even slightly appropriate in this case. Headlines such as these only serve to stoke the fire.
In order to try to cut through media Chinese whispers and rhetoric, I spoke to Liberal Democrat Councillor for Oldfield Park, Bath, Will Sandry. Will attended, and was an active part of the B&NES meeting, so I asked him for his thoughts on the deal itself, and what he thinks this means for service users in the Northeast Somerset area.
Cllr Will Sandry (Lib Dem)
Virgin Care have never had charge of a number of the services, such as social work, which are contained under this Adult Services umbrella. As I see it, this makes service users guinea pigs in this case. Would it be fair to say that this is something of a risky move on B&NES’ part?
It’s fair to describe service users as “guinea pigs” because some of the services have not been provided by a private company before, and a key element of Your Care Your Way is a redesign of services so the services themselves will change during the contact. I don’t think this is “risky” because I have faith that the wellbeing of service users will remain paramount.
During the meeting you were, along with one of your Labour counterparts, in favour of moving for a deferral of the vote so as to further scrutinise numbers you felt didn’t “stack up”, appearing to cite distraction techniques and I quote, “Jedi mind tricks”. What about the numbers and overall proposal sounded alarm bells for you?
In our meeting papers the costs of the services were listed as remaining static for 7 years. I did not have confidence that was achievable. The papers were glossy but had scant financial detail. I had also asked for details of the Virgin Care management team that would deliver the contact, but I could not get a clear answer as to how much of their time would be allocated to delivering the B&NES contact. These are the main reasons I wanted more time for scrutiny.
The most vocal reactions from the public have been almost unanimously negative; a petition, anti-privatisation websites and protest marching, as well as cries of “shame” from those who attended the meeting. We know from recent referenda and elections that small samples of public opinion may not represent the view of the community, so with that in mind, what have you and your colleagues heard from service users on the street?
Apart from the vocal reactions you describe I’ve not had any direct concerns raised by service users. I suspect that the vast majority of people don’t know or mind who delivers their care as long as it remains available to them and free at the point of use.
Conservative councillor Anthony Clarke assured the meeting that Virgin Care were not looking to make profit from this deal. I personally find it strange, and indeed improbable that a for-profit organisation isn’t looking to make a profit from a £700m deal. How is the proposed budget going to monitored and how will it be enforced by the council?
I don’t know, but would presume it will be by the Council’s Health Scrutiny Panel or the B&NES Heath and Wellbeing Board. Profit is an interesting thing. An organisation can have legitimate costs (for example the cost of using the “Virgin” brand) but not record any profits for accounting purposes. I don’t know what (if anything) Virgin Group will be charging Virgin Care for the use of the Virgin brand.
What happens if this figure is exceeded? Comparing news reports from this year, it already appears to have increased by £200m, so how does the council aim to allay concerns and potential indignation that a for-profit organisation (who controversially escape corporation tax) may possibly have a future need to utilise tax payers’ money in order to do its job?
Savings can also be made by redesigning a service to deliver the same outcomes – this was always the aim of Your Care Your Way. Ultimately if that doesn’t work I imagine that the tax payer (local or national) will pay or there will be a reduction in the levels of service available.
Has anyone shed any light on how Virgin Care plan to reinvest profits that they have assured us they aren’t trying to make?
No
We in healthcare treat patients using a risk:benefit ratio, wherein the potential risks of a treatment should be less than the benefits they could provide in order to make them viable. Given that the issues surrounding Virgin Care’s practices have been documented nationally, were these problems taken into account and considered to be outweighed by the benefits a VC-driven service could provide?
As an opposition Councillor who voted against the deal, this is a question for those who voted in favour of it. In B&NES we have good Heath and Social Care, in part because we don’t play a political game over it. Nobody would thank us for that. If it could have been proven to me that the deal was the best for our residents I would have supported it despite any personal political concerns about privatisation. Let’s hope it is a good deal for service users, but I could not be convinced about the finances of it.
Finally, Will, our whole healthcare system hinges on its patient-centred approach. Given the vote for Virgin Care, despite the vocal opposition to it, it can be logically assumed that the majority of the council feel it will bring about positive changes. What sort of changes can service users expect to see under Virgin Care? What has been proposed that betters the existing system?
I can’t speak for those who voted for the deal, but it is logical to assume they did feel it would bring about positive changes. The contact is too big to list what specific changes might be made, but I imagine any changes will attempt to keep the same beneficial outcome for service users while reducing costs.
These represent the thoughts and opinions of Cllr Sandry himself, and are not necessarily indicative of those held by his associates, or by Bath and North East Somerset Council
I must have walked past this building thousands of times over the years. I’d always admired its exterior, whose 18th century aesthetic still fits perfectly with the rest of Bath’s modernised Georgian motif. The stonework might be slightly mottled and tarnished by years of pollution, and its being surrounded by coffee shops and high-end clothing outlets *almost* detracts from the majesty the building exudes, but the Royal National Hospital for Rheumatic Diseases, nestled right in the North Somerset city’s centre still looks beautiful. I remember the public outcry when it was announced that a large chunk of the building had been sold, and subsequently leased to a novelty Mexican food chain; this building is a part of this city, not just for the patients treated within it, but for all of the residents of Bath.
Despite admiring it from the outside, I’d never consciously considered its interior. I’m not sure how many people actually have, to be honest; those I questioned had either never looked past the front doors, or had simply “heard it was quite nice” through the grapevine. I recently had the opportunity to begin to learn echocardiography at the RNHRD in Bath, and whilst I was waiting for my superiors to arrive I decided to have a look around, as it was clear from stepping through the front doors that it was a building steeped in history.
The main foyer is rather breathtaking: the original marble floors are still a prominent feature just past the reception area, paintings, such as that which is the header on this article adorn the walls and connecting the ground and first floors are beautiful, finished wood staircases that look like something out of Disney castle. I had to stop for a moment just to take it all in. Having spent a fair amount of time in hospitals, I had assumed that they (for all intents and purposes) look pretty similar; white walls, long corridors with small, commissioned pieces of generic mixed media/ abstract work hung at eye level along them, and that style of lino flooring that evokes memories of the school gymnasium, squeaking underfoot at the slightest hint of moisture on one’s shoes. Now, I’m not saying this is a bad thing (far from it), but the RNHRD has a unique character. It has charm and detail that I’ve only found in stately homes and upscale galleries. It also has history to rival these places.
Frances MacDonald, 1949
The funding for the hospital was procured predominantly via a public subscription set up by Richard (Beau) Nash in 1732. Names such as Lord Palmerston, Mr Jeremiah Pierce, and Dr William Oliver are listed as donors, as well as other local and national figures, and as a result of their capital, the building, constructed as a hospital for the sick poor opened in 1742. Built using stone gifted by local legend Ralph Allen, the then Bath General Infirmary was the first hospital to offer treatment to the entire UK, leading many to view it as a foundation of the National Health Service devised in 1948.
Locals, or those fond of UK trivia will likely already be aware of the hot springs on which Bath sits, and these were utilised in the hospital for therapeutic purposes (interestingly, Bathonians were, for a time at least, not permitted to become patients of the Infirmary, presumably because they as residents, already had a right of access to the spring waters), and these were made available to patients on condition that a fee be paid upon admission. For English patients, this was around £1.50, which later became £3, and for those from Scotland and Ireland, £3, which became £5. These sums were either paid for by the patients themselves, or on their behalf by wealthy benefactors, and covered the cost of treatment and the return home, or, in the worst case, mortality and the subsequent burial arrangements.
Patient sedan chair
A brass badge, worn by a patient whilst under hospital care
Patients were taken to the bath sites via hospital sedan chairs (designed by surgeon Archibald Cleland, subsequently dismissed for improper conduct in 1743), and impelled to wear brass badges that both identified the patient number and their ward, and to prevent drunkenness whilst out of the hospital grounds. Local landlords were forbidden from serving alcohol to patients, as it was detrimental to their recovery. Failure to adhere to this rule would have risked their licence, so it was likely seldom flouted.
The hospital was initially far smaller than its current size, with new wings and blocks being added throughout the years, including the top floor in 1793 (costing £900), renovation efforts and the implementation of additional units continuing well into the tail-end of the last century.
The Roman pavement, discovered in 1859
When the building was being extended in the late 1850’s, a Roman pavement was discovered during the foundation digging. It is dated as hailing from between AD60 and AD410 and is still in place at the bottom of the stairs to the basement level. The mosaic is still part of a larger floor and runs underneath much of the building itself.
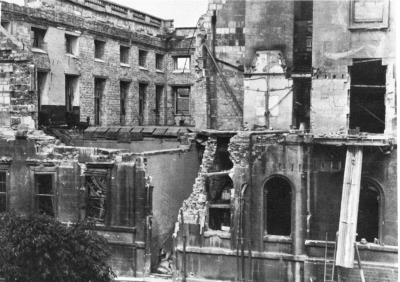
Given the tenure of the building within the city, it has seen its fair share of conflict; as well as being used to treat the wounded during the Jacobite Rebellion, the Crimean War, South African War and both World Wars I and II, it suffered damage due to ordinance during the latter conflict in 1942 wherein it received a direct hit. Despite this, however, the roughly 200 patients still within the confines of the hospital were uninjured.
Damage to the RNHRD in 1942
As far as treatment goes, the hospital has been a specialist rheumatology centre since it opened, and continues to operate as such. It offers treatments for pain management, chronic fatigue and utilises hydrotherapy as it did when it was concieved. It also functions as a research centre in these areas, encompassing both in-house studies and those of a more national variety. In addition, and I feel rather interestingly given its history with servicepersons, the centre offers specialist support to ex-military personnel, regardless of the time of onset of condition, and provides pain-management and post amputation complication therapy amongst other things.
Royal Patrons have presided over the RNHRD since its foundation, with the current President being Camilla, Duchess of Cornwall, who has been in the position since 2006. The first, in 1745, was Frederick, Prince of Wales. In 1991, the RNHRD became an NHS Trust, and was upgraded to an NHS Foundation Trust in 2005. In February 2015, the hospital was acquired by the Royal United Hospital (RUH), Bath, which now manage the centre.
The Royal National Hospital for Rheumatic Diseases truly is a wonderful hospital, and the patients who use its services do so over a number of years, crediting it with a “family feel”. Whilst researching this article, I spoke to a volunteer at the hospital, who told me of her time as a patient, both in and out, and her desire to provide a friendly ear to current service users. She told me that volunteers had relaxed her when she herself needed the hospital’s facilities, and it was that, combined with the care she was provided that inspired her to give back to the trust.
The family feel of the RNHRD was in jeopardy whilst the hospital was under considerable financial strain, but its acquisition by the RUH allowed it to continue to function with only minimal service absorption by the Royal United. This continued service will surely help the current patient base, and will enable the hospital to remain the part of the city that it has been since its conception.
This flag hangs over the museum, and was made to celebrate the 250th anniversary of the RNHRD.
Rather wonderfully, the hospital contains a museum, situated in the chapel, which outlines the history of the building and the staff and patients who have used it throughout the years. Many of the photographs found in this article were taken in the museum, and it’s full of information about the building and its history; well worth a visit if you’re in the area!
Thanks to the museum staff at the RNHRD for taking the time to talk to me and allow me to take photographs. Without them, I wouldn’t have been able to write this article.
If you’re eager to explore more, head over to Medical Heritage or visit the RNHRD homepage, and if you’re local to Bath, then be sure to drop into the Bath Medical Museum, situated within the RNHRD.
Myself and OliGS recently sat the SCST Electrocardiography Diploma and Practical Examination, so I thought I’d jot down some of my experiences in the run up, and my retrospective thoughts on the day itself.
If you’re thinking of doing it, or have your PTP finals looming, then read on, as this will give you an idea of what to expect.
I’ll start by saying this: Oli and I have NEVER been so stressed in our entire lives.
This exam was a nightmare for which to prepare; I have extensive experience in taking exams, and it is my view that they’re 50% what you know, and 50% what the examiners want you to tell them. Without having met these examiners or seen a previous paper, it was very difficult to know what to really nail, in the revision stage. The syllabus was long, detailed, and contained what seemed like an entire career’s-worth of things to learn, so we already knew it was going to be a slog, but nothing prepared us for the written paper…
Read these. Lots.
We studied, sometimes sleeplessly, for weeks. Tested each other on rare arrhythmias, read textbooks cover-to-cover (repeatedly), and watched each other’s once sunny outlooks and youthful (ahem) features rapidly wither as the examination date draw closer. It consisted of 20 multiple choice questions, 10 arrhythmia analysis and knowledge questions, and 4 full ECG analysis recordings. Some of these were almost instantly recognisable, but others were brutally difficult to analyse. The MCQs (often the most looked-forward to section of any exam) were equally tough. Those 3 hours lasted a lifetime…
We left the exam battered and bruised, but glad it was over.
But it wasn’t over. It was far from over. As well as the written paper that had almost ruined us, we had the practical exam to do as well.
We had made sure that during our post-ECG placements we still got ourselves in the clinic so as to keep everything fresh, as performing a perfect ECG is not like riding a bicycle.
The last attempt before test day
It turns out that this was the correct call, as was practicing on one another in the hotel the evening before the exam; the margin for error in the exam is 2mm(!) Anyone who’s had an informal assessment, or had their Direct Observed Practice scrutinised whilst training knows that it’s very easy to second-guess when it comes to electrode placement, and despite having 20 minutes to complete the whole thing, this timeframe becomes devastatingly short once you’re in there. It’s a clinical assessment, so one needs to complete the necessary ID checks, explain the procedure to the patient AND to the examiners (i.e. in two different ways), perform it whist answering questions, and then complete a verbal examination.
Three hours after we had finished the written paper, we were called to attempt our practical exam. There were ashen faces all around. Some were on those still waiting for their number to be called as ours had just been, others had been told that their 2 attempts had been unsuccessful. Neither of us were looking forward to this. Now, given that I’ve already stated that each electrode is allowed to deviate only 2mm from the precise, gold standard location, the internet-purchased electrodes pictured in the above image would be somewhat unfair, right? It seems that the examination board concur, as they provide some rather cool, transparent electrodes complete with crosshairs. They doesn’t make it easier, per se, but they certainly go some way eliminate that lingering trepidation when it comes to deciding you’re happy with your placement and ready for judgement.
Crosshair emblazoned electrodes(!)
I opted for the “all at once” technique: I explained everything to the patient before I started, gained consent, then explained everything I was doing as I went along. Once was put simply to the patient, then once to the examiners, using correct terminology. I paid extra special attention to V1, V2 and V4, as my patient had a particularly wide sternum, so I wanted to be totally sure that I had the sternal border, especially given the electrodes were rather far apart when placed and looked slightly odd to me. After I took a step back and looked at my work, I was incredibly tempted to move the aforementioned electrodes, but either due to fear, fatigue, or a combination of the two, I decided to leave them as they were, opting to go with my initial judgement. After that, I waited.
I’m not entirely sure how the placements are measured, as candidates are asked to leave the room whilst they are checked by two examiners. I heard someone mentioning special rulers, but I didn’t get a look at them (it’s all very cloak and dagger), in any event, you’re called back into the room and, in my case at least, informed of your passing or failing grade. I’m pleased to report that I passed on the first attempt, which as I’m sure you can imagine, was a tremendous relief; I lost my cool somewhat, and expressed my joy rather loudly, as I was informed I wouldn’t have to do it again. Oli soon found me in the waiting area and, grinning wildly, slapped me on the back and hissed “YESSSSS!” before promptly throwing himself into a chair. It was over, and we were victorious.
We didn’t speak too much about it, on the way home, but in the couple of days that have passed since the exam, we both feel a tremendous sense of pride that we actually did it, and did it successfully. If I were to give you all some advice, it would be the following:
Be prepared for anything and everything, including waiting around for a long while
Practice analysing ECGs until you hate them
Practice performing ECGs until you hate them
Go with your gut as much as you can during the practical exam
Bring lunch
Don’t under ANY circumstances, stay at the Ibis Hotel in Birmingham’s Chinatown district (I can’t stress this enough because it backs onto a nightclub that doesn’t stop playing the most bass-heavy music until the wee hours of the morning)