

Literally means heart (cardio) muscle (myo) disease (pathy) and describes a condition that impairs the heart’s ability to expel blood efficiently, resulting in a reduced cardiac output and flow.
There are three principal types;
- Dilated Cardiomyopathy (DCM)
- Hypertrophic Cardiomyopathy (HCM)
- Restrictive Cardiomyopathy (RCM)
Mortality is increased, with a 2 year survival of 50%
Dilated Cardiomyopathy
Occurs as the result of a compensatory mechanism to combat a sustained decrease in cardiac output.
Causes are generally idiopathic, but can be the result of infarct, genetic or sometimes due to pregnancy.
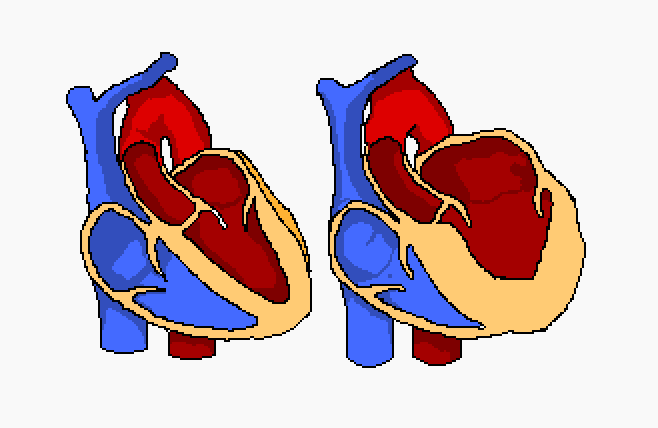
Structurally, it looks something like the below illustration.

The dilation of the ventricle(s) causes a loss of systolic function, so the heart’s ability to contract is sub-optimal.
The structural remodelling of the ventricles allows a greater volume of blood to enter them, meaning more can be ejected, and cardiac output is, initially, maintained.
The dilation is exacerbated however, due to the unwanted volume of blood that remains in ventricles during diastole. The diagram above shows the thinned cardiac muscle around the left ventricle, so whilst the heart is still contracting, the contraction is insufficient to expel the usual 50-75% of blood achieved with normal ejection (a decreased ejection fraction. In DCM, this is measured as <40%). Eventually, this decreased ejection fraction will affect also, the atria, as a result of the “backlog” of blood remaining in the ventricles.
The maximal dilation of the cardiac chambers, causes the symptoms of heart failure:
- Chest pain
- Syncope
- Ankle oedema
- Fatigue
ECG features:
No features are exclusive to DCM, but there can be found clues to its presence;
- LVH
- Left axis deviation
- LAE
- Bundle branch block
- Poor R wave progression
Hypertrophic Cardiomyopathy
Causes of HCM are largely unknown, but there are numerous things that can contribute to it; inflammatory infection, uncontrolled hypertension, alcoholism, “House MD” favourite; Lupus, genetics and pregnancy.
HCM is the most prolific cause of sudden cardiac death in young athletes and is frequently asymptomatic until death, so screening is important in picking it up. These screenings generally involve a thorough patient history and physical examination, including ECG, but these practices catch a disproportionally low number of HCM cases. The gold standard, catching circa 80% ooh them, is echocardiography, specifically showing the increased muscle mass and Doppler analysis of a systolic ejection murmur.
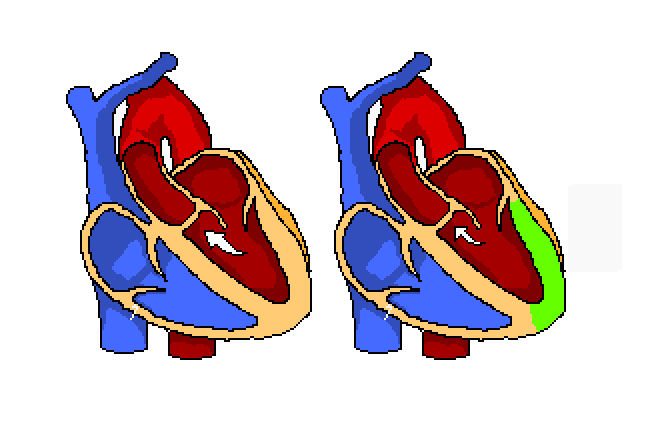
When one of the above factors gives rise to a decrease in contractility, this causes a size increase in cardiac myocytes which, in turn, alters their alignment (known as myocardial disarray). These factors cause an increase in mass of the myocardium and ventricular diastolic dysfunction resulting from impaired relaxation and filling of the stiff and hypertrophied left ventricle. In addition, thickened walls and narrowed lumens can be found in the coronary arteries and occasional mitral regurgitation within the heart.
A degree of hypertrophy is the chief associated abnormality in HCM, and it is usually asymmetrical, affecting the left heart and around 2/3 of the septum.
Reduced internal ventricular area results in a decrease in outflow, this is further present, as can be seen in the above diagram, by the obstruction of the outflow tract from the ventricle.
So, to go back to basics, the decrease in contractility, cause the ventricular ejection fraction to decrease. The heart tries to compensate for this by increasing its muscle mass, but this effectively shrinks the ventricles, lessening the volume of blood able to be pumped into them.
The hypertrophied IV septum causes an intermittent outflow obstruction, depending on how hard the HCM heart is working, and the current stage of the cardiac cycle. At a normal heart rate, this obstruction isn’t so pronounced, but at higher heart rates, the systolic function causes the tract to be sufficiently narrows so as to cause a blockage. Combined with the already lessened volume of blood entering the ventricle in the first place, the ejected volume is sometimes severely diminished.
Infarct, ischaemia and arrhythmia are common in HCM.
Symptoms, if present, can include;
- Chest pain
- Palpitations
- Exceptional syncope
- Dyspnoea
ECG features:
- LVH
- LAE
- Deep, pronounced Q waves in the lateral and inferior leads
- V5, V6, I, aVL
- II, III, aVF
- Very pronounced T wave inversion in Precordial lead trace.
- Features of arrhythmic activity, such as AF, may indicate the underlying pathology
Restrictive Cardiomyopathy
The rarest of the three major cardiomyopathies, deposits within or fibrosis of the myocardium causes stiffening. This reduces the heart’s ability to relax, therefore giving rise to diastolic dysfunction.
As with the other myopathies outlined on this page, RCM exhibits a loss of cardiac output, but where systolic mechanics are normal, it is the impaired filling of the ventricles that causes the loss.
ECG features:
- Low QRS voltage
- T wave abnormalities
- Arrhythmias
- Bundle branch blocks
References:
Topol, E., Califf, R., Prystowsky, E., Thomas, J., Thompson., (2007) Textbook of Cardiovascular Medicine. 3rd Ed. Philedelphia: Lippincott Williams and Wilkins
Jenkins, D., Gerred, S., (2011) ECGs by Example. 3rd Ed. London: Elsevier Churchill Livingstone

