

The normal conduction pathway of the heart, (wherein depolarisation begins at the SA node and spreads to the AVN, HIS bundle and then through the bundle branches and Purkinje system) can become hindered or blocked.
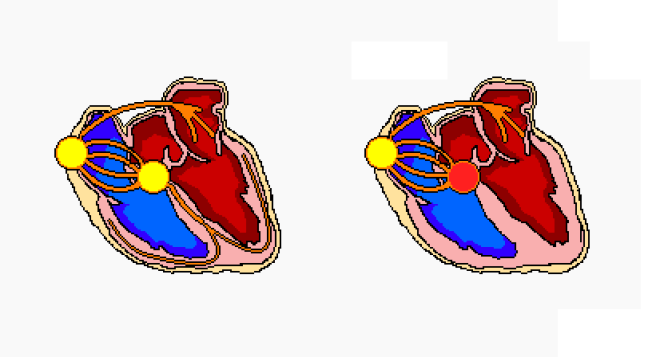
These blocks should be, in theory at least, relatively obvious on the ECG trace, when one considers the properties of a normal trace; a block in the conduction pathway between the SA and AV nodes will result in a change in PR interval, giving one that is longer than the normal 220ms in some cases, and an absence of a QRS in others.
When assessing AV block, study the leads with the most prominent P waves, which are normally V1 or Lead II.
In the case of 3rd Degree Heart Block, assess PR interval in all of the leads to look for a lack of consistency.
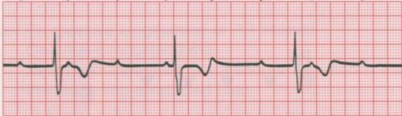
1st Degree AV Block
- Each depolarisation reaches the ventricles
- P → QRS
- The block results in a delay
- PR interval >220ms/6 small squares
2nd Degree AV Block
- Intermittent non-conduction of the depolarisation signal through the AV node or HIS bundle

- Progressive prolongation of the PR interval
- Results in dropped ventricular beat
- P → QRS, P →→ QRS, P→→→, P → QRS
- Results in dropped ventricular beat
- PR interval:
- Longest before the dropped beat
- Shortest immediately after dropped beat
- Relatively constant P-P interval
- R-R interval shortens progressively
- P wave may present with a T wave distortion
- Failure at AV node-level
- Progressive exhaustion of AV cells, resulting in non-conduction

- Sporadic non-conduction or depolarisation wave through AV node
- Results in dropped beat
- P → QRS, P → QRS, P →, P → QRS
- Results in dropped beat
- PR interval remains constant
- R-R interval is a multiple of the preceding dropped beat
- Double after 1 dropped beat, Treble for 2…
- P:QRS may display a pattern
- 2:1, 3:1, 4:1 P waves for every QRS complex
- QRS complexes can present as broad (75% of cases) or narrow
Pathophysiology:
- Failure at HIS-Purkinje level
- Sudden and unexpected failure of cells to conduct
- Usually exists with existing LBB or Bifascicular Block
- Can cause sudden cardiac death
- Can progress to 3rd Degree HB
3rd Degree AV Block (Complete)
Features:
- Bradycardia
- AV dissociation
- None of the SA impulses are conducted through AV node
- Atrial rate and ventricular rate have no relationship
- Ventricular perfusion resulting from escape rhythm in ventricular muscle
- Atrial rate and ventricular rate have no relationship
Pathophysiology:
- Chronic presentation:
- Fibrosis around HIS bundle
- Acute presentation:
- Stems from MI
- Thought to be due to AV nodal-level failure, as with Mobitz I
AV blocks are usually the result of:
- Ischaemia
- Pharmacological agents
- Conduction-degrading conditions
References:
Wagner, GS. Marriott’s Practical Electrocardiography (11th edition), Lippincott Williams & Wilkins 2007.
Hampton, JR. The ECG Made Easy (8th edition), Churchill Livingstone 2013.

