

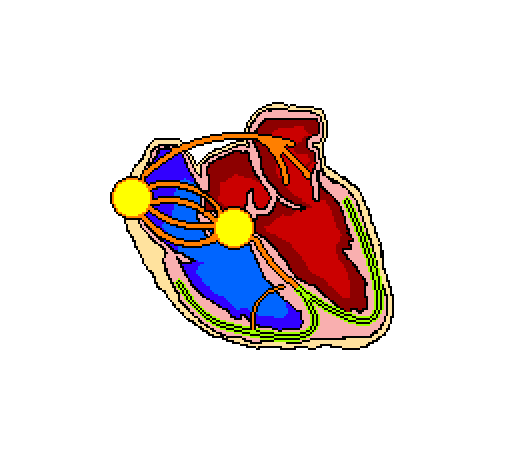
 The left and right bundle branches (LBB & RBB) are the areas of the cardiac conduction system responsible for carrying the depolarisation signal to the ventricles.
The left and right bundle branches (LBB & RBB) are the areas of the cardiac conduction system responsible for carrying the depolarisation signal to the ventricles.
They allow for the rapid activation of both ventricles simultaneously.
The are supplied with blood via the coronary arteries, predominantly;
The left anterior descending coronary artery supplies the LBB, and it also provides most of the supply to the RBB, albeit it the septa branches. In addition to this, the circumflex coronary provides some supply.
The RBB and LBB are a division of the Bundle of His. The LBB makes a further three divisions:
- Septal fascicle
- Innervates the interventricular septum
- Anterior fascicle
- Innervates the anterior and superior LV
- Posterior fascicle
- Innervates the posterior and inferior LV
A block of impulse conduction through either BB is termed a bundle branch block, but if one or more of the fascicles is blocked, it is known as a hemiblock.
Thus, possible blocking sites are:
- Right Bundle Branch
- RBBB
- Left Bundle Branch
- LBBB
- Left Anterior Fascicle
- Left Anterior Hemiblock
- Left Posterior Fascicle
- Left Anterior Hemiblock
Purkinje conduction is not assessable on an ECG, due to the small amplitudes of the signals.
Bundle Branch Block ECG Characteristics
- QRS complex ≥0.12s
- Notched or slurred in chest leads.
- Ventricles depolarising out of sync
- Notched or slurred in chest leads.

Incomplete BBB denotes a slow in conduction through the bundle branches, so presents with a QRS <0.12s

ICBBB is a common and normal variant in children
Right Bundle Branch Block
- Conduction does not commence until the LV is almost fully depolarised
- Tall, notched QRS complexes
- V1 , V2
- Slurred S waves
- I, V5 , V6
Left Bundle Branch Block
- Dominant S wave
- V1
- Tall, notched QRS complexes
- V5 , V6
- Often synonymous with LAD
LBBB Pathophysiology
- Often a marker of heart disease
- Hypertension
- Valvular disease
- CAD
- Post surgery finding
- Can occur with age
- Can be a normal variant, although this is rare
Hemiblocks
Left Anterior

- LAD
- Usually ≥-60
- Small Q waves
- I, aVL
- Small R waves
- II, III, aVF
- R wave peak >0.045s
- aVL
- Increased QRS voltage
- Limb leads
Left Posterior

- RAD
- Usually ≥ 120
- Small Q waves
- II, III, aVF
- Small R waves
- I, aVL
- R wave peak >0.045s
- aVF
- Increased QRS voltage
- Limb leads
Bifascicular Block
- A blockage of either:
- LAD
- RBBB & LAH
- Notched QRS in V1
- QRS >0.12s
- Slurred S waves in I, V6
- RBBB & LPH
- RAD
- RBBB features
- Q waves in III
Ref:
unmc.edu
lifeinthefastlane.com

