
As part of our course we often perform ECG’s on one another to enhance and refine our practical ECG skills. During a practical recently I volunteered to be the patient so that my fellow students could practice their electrode placement skills; whilst being filmed and critiqued by others. The group universally agreed in the value of this experience, despite the fact it felt strange performing an ECG to an audience of your friends whilst being filmed in an artificial clinical environment. After everyone had practiced we printed of a recording of my ECG. Our lecturer, whom is a senior physiologist, explained that we would as a class analyse the ECG in our following lecture.
Upon the analysis of my ECG, my lecturer broke the news to me that I had left ventricular hypertrophy (LVH) with sinus bradycardia. Considering the previous lectures we’d had on LVH and its clinical significance I was pretty scared few a seconds or so. He then thankfully reassured me that in my case this was completely normal. My lecturer emphasised the importance of always combining your ECG analysis and findings within the context of your patient.
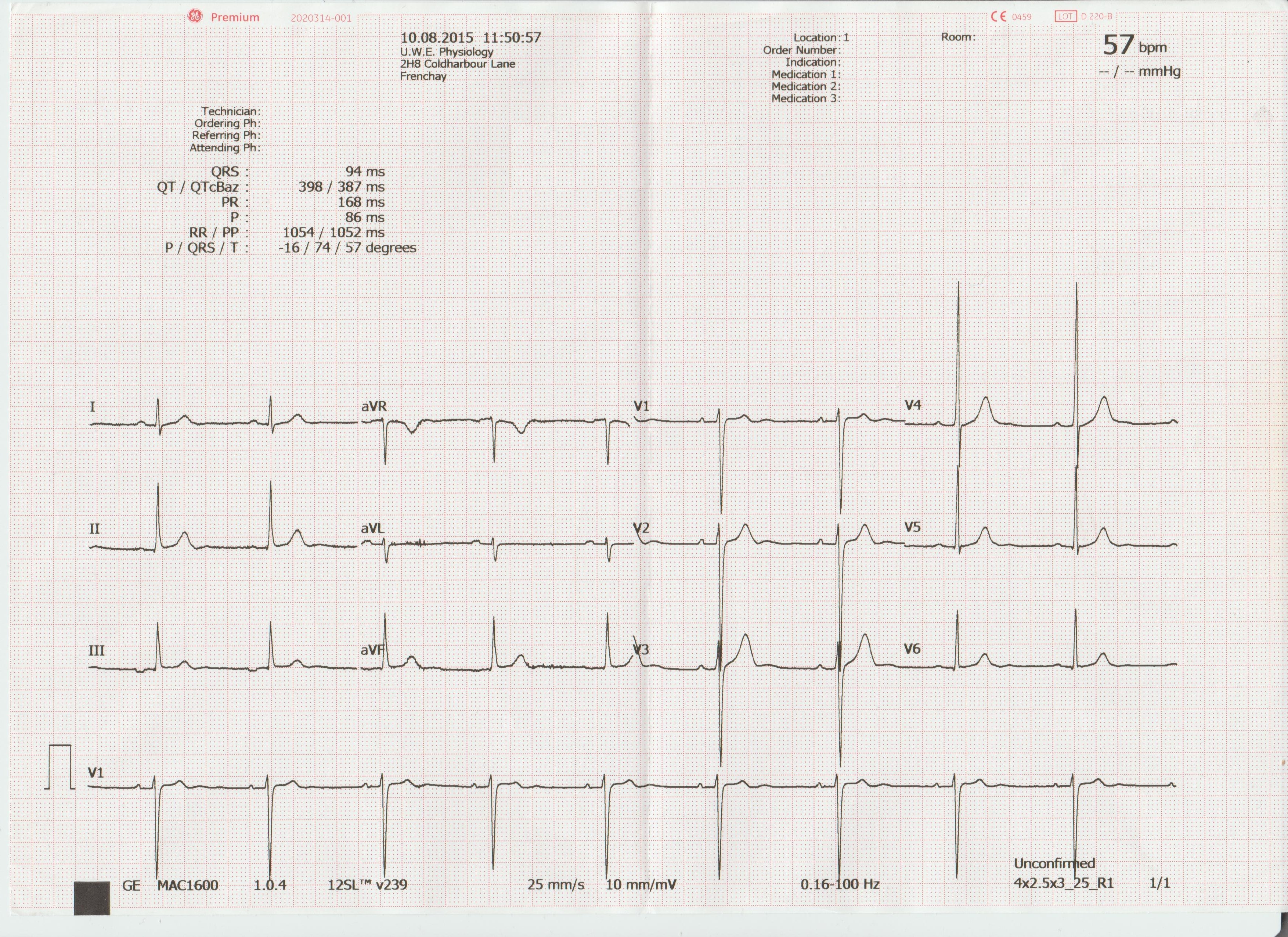
He explained my athletic physique (his words) and my age were enough to convince him that my development of LVH was not due to pathological reasons but that of heart remodeling as a result of prolonged physical conditioning. If presented with a 30 stone, 60 year old male, with LVH, or a 70 year old sinus bradycardic female ticking a long at 50 bpm and suffers occasional syncope; this would not fit as a normal finding in the context of these patients.
This practical highlighted the importance of always putting your ECG findings in the context of your patient and the normal ECG variants that may be encountered. The patients we see will be varied. They will be of different genders, ethnicities, ages, physical condition, possibly even pregnant. All these groups will produce significant normal variants in their ECG’s. These factors must always be taken into consideration when assessing the significance of your findings. Is your patient bradycardic and symptomatic suffering frequent dizzy spells or are they a young physically conditioned adult. We will be posting articles shortly on the normal variants expected in some of these patient demographics.
What is LVH
LVH is an increase in size and proportion of ventricular myocardium (in this case specifically the left ventricular myocardium). This can occur in any chamber of the heart but is most commonly found in the LV.
How is LVH diagnosed on an ECG
Most trained operators will spot signs of LVH relatively quickly on a ECG recording as it will be common that precordial ventricular tracings will overlap one another requiring a reduction in gain settings.
However, the Sokolow Lyon criteria is correct method of choice. This involves measuring the amplitude of the S wave in V1 and adding it to the R wave amplitude in V5 OR 6 (whichever bigger). If the sum amplitude is greater than 3.5mV LVH is suspected.
To calculate right ventricular hypertrophy (RVH): Amplitude of R wave in V1 + S wave V5 or 6. If the sum amplitude is greater than or equal to 1.1mV RVH is suspected.
However, an ECG alone cannot determine the extent of hypertrophy and its clinical consequence. An echo-cardiogram would be required to ascertain this.
Causes of LVH
LVH is a result of increased demand put on the LV to increase cardiac output. Over prolonged periods of time this increases cardiomyocyte size. As discussed earlier, this increased CO demand could be the result of exercise, and therefore sustained activity levels could lead to LVH. The upshot of this is that for every heart contraction the ventricles can force out a greater volume of blood for every beat (stroke vol) reducing the demand on the heart to supply cardiac output at rest. For this reason athletes with LVH will have a lower resting HR (sinus bradycardia).
However, there are also many pathological reasons for developing LVH, all of which result in pressure overload in the LV increasing its resting workload.
Some of the most common pathologies associated with LVH are as follows:
• Hypertension (most common cause)
• Aortic stenosis
• Aortic regurgitation
• Mitral regurgitation
• Coarctation of the aorta
• Hypertrophic cardiomyopathy
As LV hypertrophy develops, the myocardium can become so thickened that it begins to inhibit the filling of the LV reducing cardiac output leading to increased risk of mortality.
In my next article I will be looking further into some of the pathological causes of LVH and their clinical significance.
Ref:
http://lifeinthefastlane.com/ecg-library/basics/left-ventricular-hypertrophy/
