In amongst busy shifts, I’ve been tweeting about HCS Week 2018, and chatting to other scientists about their experiences. Yesterday, I tweeted a picture of Helen, a specialist Echocardiographer, whilst she was hard at work analysing pulse wave data, and today I’m sharing the answers she gave to a couple of questions I asked her about what she remembers about the history of her job in her 30 years of experience, and her feelings on the changes she’s seen over the years.
With 30 years under your belt, you must have noticed changes in your profession. What’s different now, compared with when you started?
Firstly, my job title has changed. I was a “Cardiac Technician” and began as a student working in Cardio-Respiratory, with a full-time, guaranteed job at the end of my training. I studied on a day-release basis for an ONC then HNC, eventually topping up to BSc when this became compulsory.
Technology has had a big impact on advancement of procedures, which is better for patient quality of life, etc; Cardiac Techs performed all the ECG’s in the hospital, carrying a crash bleep for A&E, and now, of course, there is provision for ECG’s on every ward and dept.
Procedures such as angioplasty and bi-vent pacemakers were not as widely available, either; most CAD patients went on to undergo CABG and only relatively basic bradycardia devices were on offer. Obviously this is all change now.
Alongside this, we are now much busier than ever before and our roles have changed massively. We now carry out duties which years ago only consultants could do. I think this is good for everyone but does mean we have much more responsibility, in addition to greater autonomy. We are, however, still part of a team, which is vital to remember.
Did you have any reservations about the changing nature of your specialism?
I used to worry that becoming more busy and more academic would threaten our profession, that less qualified staff would have to take on more of our roles. Fortunately, routes into this career seem to be more widely available and thus, accessible. Emphasis seems to be more about finding the right person for the job, and training is focused, usually by specialist Scientists who understand the needs of both the students and patients.
It’s important to realise that anyone can be shown how to perform an ECG or assist in a cath lab, but qualities such as initiative, kindness and compassion are inherent traits which cannot be taught, and are absolutely vital in this profession.
Studying ECG can be one hell of a mountain to climb, especially when you’re at the novice level of cardiac education. Due to how vital it is, it’s imperative that you can not only make the distinction between Mobitz II AV Block and sinus arrhythmia, but also understand the intricacies of the cardiac conduction behind them, and all of the other rhythm abnormalities. Learning these things like the back of your hand is one thing, but combining all that knowledge is, at times, overwhelming. So after 12 months of scouring the internet, trying to find a decent cardiac anatomy and 12-lead ECG simulation tool, I was over the moon to stumble upon Epicardio Simulation; a cardiac electrophysiology tutorial application, developed by Epicardio ltd.
The program is available in 3 main forms; Epicardio ECG, ECG and Pacing, and 3-day trial. As I don’t have £149 kicking around (the price of the basic ECGcentric offering), I can’t review the full version and all of its features, but the 3 day trial version (which is £0), is well within my price range. Thus, I shall only be commenting on the features with which I have been able to sample.
Thankfully, the collection of features available to trial version users is still extensive, so I have lots to cover, and perhaps I’ll spring for the full version when funds allow. The question is: does the trial impress enough to warrant the large expense? Let’s investigate further:
Almost as soon as you open Epicardio, the vibrant display hits you; a large, anatomically accurate heart fills most of the screen as colourful depolarisation waves travel across the atria, and down through the ventricles. The live single lead ECG tracks with concordance, and the right hand menu buttons are nicely presented and clearly display exactly what they do.
Depolarisation mechanics can be viewed through the heart as a whole, or each section on its own. Atria, ventricles, bundle branches and coronaries, can all be viewed independently whilst depolarisation occurs, so it’s possible to learn how the various components of the cardiac system operate during each cycle.
Further structural overlays can be added, in the form of the vena cava, thoracic cage and a translucent torso, further adding to the ability to understand the heart’s positioning in humans.
The electrical readout on the lower region of the screen comes with the option of cycling through all 12 leads on the standard ECG, individually, but as well the real time single lead ECG, users can also activate a live 12-lead, which again updates in real time with each cardiac cycle. This mode itself allows for different viewing styles, including the layout presented on most standard ECG printouts, which is perfect for students. It also features all the subtle morphology differences and minor, unavoidable muscle tremors that one would find on a real ECG recording. Calipers are a welcome feature, too, and they work well in Epicardio, allowing for measurements that students will definitely have to become proficient in throughout training.
Further customisation options are numerous; the colours of the depolarisation waves are changeable, as is the colour of the backdrop. Rather than simply offering pre-set rhythms, Epicardio allows you to manually alter heart rate, and, possibly more importantly, AV delay, so it’s possible to visibly alter the depolarisation wave on the beating heart in the centre of the screen, and see the live trace display a prolonged PR interval.
A most welcome feature is the electrode view option. A click on this button brings up a moving image of the heart within the thorax, and the standard precordial electrode sites. These electrodes can be moved anywhere and the real-time result displayed on the recorded trace, so it’s rather nice to be able to explore the difference in the voltage/time graph that occurs with electrode misplacement.
A defibrillator option allows you to shock the heart, although this was of limited use to me, as I did not have access to the fibrillatory rhythms that come with the paid version, but the artificial pacemaker below it allows the user to alter pacing pulses and observe the changes on the ECG.
My issues with Epicardio range from those that exist simply because the version I tried is restricted, to those that are nought but minor niggles, so I shall focus on those minor niggles, as oppose to content I simply have not paid to access.
The ECG trace, whilst being incredibly customisable, would feel much more authentic if it were set against a proportional image of standard ECG paper; being able to view the trace against the background most students will see throughout studies would be a great primer in the early days of study, and considering the trace speed is adjustable, I was disappointed it wasn’t a feature.
The option buttons look lovely, offer genuine function and, once you’ve been through the tutorial and played around with them, make perfect sense. It would perhaps be helpful if a brief explanation appeared when the mouse pointer was placed over each one, however, as it was a struggle remembering what the more vague options actually did, especially for the first few hours of using the program.
However, as I stated, these are only minor gripes. Epicardio is a wonderful and genuinely fun bit of software to use. I’ve got a feel for how beneficial having this in the beginning of my studies would have been. The layout, options, functionality and simplicity of using Epicardio are all near-perfect, so I can’t wait to get a hold of the full version, complete with pacemaker-specific options. If you have a spare weekend, then follow the link at the top of the page, and download the free trial. If you have a spare £149/£215, then follow the same link and download the full version, as if it’s provides even 50% more features than the demo, I can be certain it’s worth it.
I had the rather marvellous opportunity today; spending a day in cardiac theatres and, under the guidance and tutelage of two cardiac surgeons and an anaesthetist, learning the processes and methodologies behind CABG and MV repair.
I arrived at the Bristol Royal Infirmary surgical centre at 7:45am and was quickly changed into some scrubs and inducted into the OR’s team: three surgeons, two anaesthetists, one perfusionist and a selection of nurses both scrub, and regular. It was clear to me that each of these individuals knew one another well, just by the way they talked to each other; everyone seemed at ease with the rest of their colleagues. It turns out, I was right. Many of them knew each other from other hospitals, university or simply having been mentored by each other during training. This camaraderie bled into the surgery, as each team member knew not only their role, but that of the others, also, so equipment was passed over or set up without being requested, making for a seamless procedure.
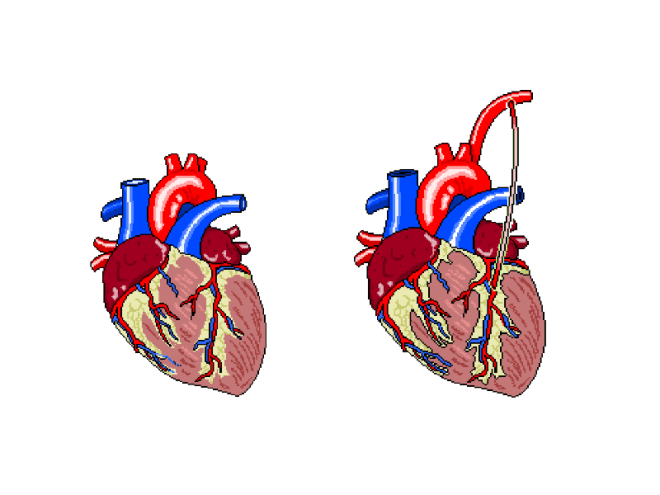
The patient was, until the last year or so, a very fit and active 79y/o, who had suffered from AF for at least 10 years, and had developed a stenosed left anterior descending coronary artery as a result. In addition, echo had shown a severe mitral regurgitation due to valvular prolapse. The procedure would attempt to bypass the LAD using the left internal mammary artery (LIMA), as shown below.
Figure 1: The left internal mammary artery (shown in situ on the right) is relocated from the chest wall to bypass the stenosed section of the LAD.
The plan was to perform the bypass graft, and then set about repairing the damaged mitral valve.
After the patient’s ID and contraindicators had been checked, the anaethetists set about carefully monitoring their respiratory and cardiovascular function as the GA took effect. The ECG, arterial and venous pressure traces were available on lots of screens around the rooms, as whilst they must be monitored all of the time, it becomes particularly important to keep an eye on the given values as the heart is both stopped and re-started.
Interestingly, I noticed a pattern in conversation with each patient throughout the day, as the anaesthetic was administered. The patient was asked to think of their favourite place and the team then asked where that place was. Each time, this was met with silence, but just to make sure, the patient was always asked if they were warm enough. When no answer was forthcoming, they were wheeled into the theatre room proper.
Not everyone on the team was scrubbed up and sterilised, as obviously some would not be required to touch the patient, and others would be required to fetch replacement equipment should it be needed. This created a “sterile field” around the operating table, so only sterile members of staff were permitted within it.
After 1 hour and a whole heap of sterile gowns and drapes were applied over the patient, with only a small window showing the surgical site, the operation began.
Step 1 required access to the thoracic cavity. In case of blood splatter, masks fitted with facial protection were supplied to myself and the other team members who would be in the direct vicinity of the patient when the chest was opened.
An incision was made as illustrated below. This is known as a median sternotomy, and extends from the sternal notch to the xyphoid process. In order to progress past the sternum, an oscillating saw is used to cut throught it. There is a surprising amount of finesse involved in this stage, despite how much pressure is required and as a result, how brutal it appears.
The incision is deepened and cauterised until it travels through the pericardium, so as to allow access to the heart and, after the bleeding vessels around the wound are cauterised, a finochietto retractor is used to hold the sternum open. During this time, the LIMA is found and carefully removed from the chest wall. It is then held in an accessible place with forceps, to be used later.
Lung and cardiac function is transfered to a cardiopulmonary bypass machine, which allows both the heart and lungs to be stopped/emptied, allowing even greater access to the heart due to the lack of lung obstruction, and intricate work to be perfomed whilst the heart is not beating.
The cardiopulmonary bypass apparatus purifies the blood that passes through it from the patient via cannulas placed in the heart and pumps it back, thereby doing the work of the heart and lungs. The heart is fed nutrients at the same time, so as to keep it healthy for the extended period of inactivity. This method of on-pump surgery is known to be incredibly safe- between 1 and 2% of high risk patients will suffer adverse effects as a result of the treatment, and surgical teams are well versed in assessing this via risk factors.
Once the LAD has been correctly identified, an incision is made, creating an opening that roughly matches the size of the end of the LIMA, and the two are stitched together using sutures made of polypropylene,which are no thicker than a human hair, yet can withstand the pressure that would be required to rupture a healthy vessel. To test the suture site, blood is passed through the vessel, and in the event of any gaps in the connection, this blood will be seen outside of the join, which can then be further secured as necessary.
The process, whilst quick to document, was a long one, as each step of the technique was scrutinised carefully before considered complete. In addition, each stitch required at least two people directly, to exact it; one to add the suture, and the rest to support the structures surrounding it.
The second stage of this case was the mitral valve repair, which was in itself a multi-stepped procedure. It is possible to repair a damaged mitral valve using less invasive, keyhole methods, but due to the need for a bypass graft, this wasn’t an option this time.
After gaining access to the valve itself, via an incision in the left atrium, the condition of the valve leaflets is assessed. This particular patient’s posterior leaflet had a prolapsing middle scallop, which meant that the below procedure was necessary to repair it.
The process off attaching the ring was a long one, involving a lot of organisation and intricate knotting. The sutures are applied to both the ring and the valve, the latter is then gently pushed down the threads and into place. These suture strings are then tied off and cut.
Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.
When performing the annuloplasty removed the surplus anterior leaflet, it took with it a tendineae chordeae, so in order to stabilise it further, an artificial heart string (made of Gore-Tex) was attached to the leaflet and papillary muscle.
A final transesophageal echo was performed, to assess the level of air still present in the heart, and to then assess the function of the repaired mitral valve, and after all of this was successfully accomplished, the long task to gently remove all of the cannulas that were used to bypass the cardiopulmonary system were begun to be removed. Each chamber was sutured in sequence, and the corresponding section of the perfusion apparatus turned off. All of this time, the anaesthetist monitored the patient’s drug infusions and every member of the team monitored pressure and ECG traces. This was still going on whilst the SpR set about cauterising vessels and wiring the sternum before pulling it back together. None of this section of the procedure involved any real finesse; pulling the wires taut so as to close the chest cavity is a test of strength. Each pull caused the patient to move for the first time since coming into the theatre, so I guess that was why it was the only section of the surgery that almost made me wince (something the theatre lead noticed and laughed about). Once it was done, the multiple layers of sutures were applied to seal the surface wound and the patient was taken to recovery.
In all honesty, the most difficult part for me, was in standing for so long. This was echoed by the surgeons, who said that they always felt backed up by their colleagues, so they felt confident that the procedure itself would go well, but standing, often in an unnatural position for so six hours at a time played havoc with their backs and legs. The anaesthetists, being required fully at the beginning and the end of the surgery, spent a great deal of time sat waiting, save for occasionally changing an infusion as and when required. The people working solidly were the surgeons and the scrub nurse, but even the surgeons swapped roles, observed one another without participating, and even took breaks periodically. None of this diminishes any one role, however; each member of the team was required, be it constantly or otherwise, and when one was needed, it took a single word for everyone in the room to know what was required, and by whom. Despite the procedure itself being amazing, it was the mechanical and seamless nature of the professionals in the room that was the most astounding part of the day.
Smartphone and tablet technology is advancing at a rapid rate, so it should come as no surprise that it is being used for a variety of different purposes. Healthcare companies are finding novel ways to encourage patients to take charge of their own health; peripherals allow for BP measurement and three lead ECG monitoring in one’s own home, and it’s possible to measure your heart rate at rest and during exercise now, with software that comes as a pre-installed fitness suite on most modern devices.
It stands to reason, then, that these same companies would create clinical grade applications and device extensions that would benefit practitioners, also. I covered the use of Google Glass in revascularisation, already, but another device is making its way to the market at the moment, too; mobile ultrasound.
After unveiling it in 2014, Philips were granted FDA approval of their Luimfy system only a couple of weeks ago and have announced that it is now available for purchase in the US.
A $199 per month subscription, an Android phone/tablet and a micro USB probe are all you need, as the app and it’s peripheral are designed to work with compatible devices off-the-shelf.
In its current form, the scanning app allows practitioners to examine the gall bladder, abdomen and lungs, in addition to having obstetric, vascular, superficial, musculoskeletal and soft tissue functionality, so the device isn’t suitable for echocardiography, but I’m certain that in the future, given the power already available in modern devices, it’s a real possibility.
In UK hospitals, where space is a deciding factor for treatment options, having an ultrasound monitor that can fit in a small case would be a real boon. Emergency and critical care ultrasound is actually what the system was designed for, so it makes sense that the most obvious impact relates to time and accessibility.
Streamlining the healthcare process is paramount, and the fact that this system is based around an app could be a real advantage. The images gained by the practitioner can be shared via the cloud, so the network of professionals involved with one patient can have near instant access to the relevant materials needed for diagnosis. Philips could also provide continued software support and provide updates based on user feedback, without the need for engineer call outs.
Now, I’m no app developer (I’m trying. It’s rather complex…), but I do use them, so I can identify some common problems in cloud storage and functionality.
Firstly, as this is an Android app, it may present issues in performance across devices. There are a number of latency issues with apps for this OS and further issues regarding app performance in general from one device to another, especially if the base OS differs slightly between manufacturers (if you’ve tried to compare performance between Samsung and Google Nexus, you’ll know what I mean). In this case, Philips would have to be fairly on the ball with their customer support, especially given the subscription costs for practitioners.
I guess the issue with cloud storage brings us to patient confidentiality, as the last couple of years have seen some high profile cloud hacks leak “sensitive” data to the public, but many hospitals are already digital, so surely it’s a case of ensuring the level of security is appropriate.
As far as echo goes, the advantage of switchable probes and live, cloud updating comes into its own; echo features could be added with an update, in theory. It’s a case of making it happen. It’s unlikely, but if I ever get a chance to try one, I’ll make sure to tell you of my experience.
It has been brought to my attention that I didn’t word some of my last post particularly well. Upon looking this over, this is indeed the case.
It was not my intention to convey that healthcare scientists need not perform ECGs I intended to imply that whilst on my last placement, physiologists did not perform them, it was the responsibility of the A.T.O. hence, this is what led my mentor to say what they did regarding newly qualified and echo. This may not be the case across all trusts.
I neglected to include that due to the advanced nature of the practise of echocardiography, it is not featured in the PTP program. (This is good news for me and anyone else currently studying this degree, as I shudder to think of the extra workload that would be associated with it).
If in future I make an error such as this, let me know and I shall endeavour to rectify it.
Many thanks,
TSP.
ORIGINAL POST:
Having seen what trust-employed cardiac physiologists are required to do, it seems rather strange to me that echocardiography isn’t really taught in either the PTP or STP programmes. By all accounts, it’s touched upon in the final stretch of the STP pathway, but not in a comprehensive manner. Assistant Technical Officers perform the vast majority of ECGs in my trust, so it isn’t necessary for qualified healthcare scientists to be placed in that area. My mentor told me that her cardiology department needs echocardiographers and that the discipline is underinstructed by the universities. Bear in mind this is only because it isn’t a part of the syllabus as it’s not currently required by the framework of Modernising Scientific Careers.
As a result, the trust I have been stationed in has taken to rounding up the students and providing its own echo tutorials after the working day is finished.
This is a great idea and is beyond the call of duty for the department physiologists, but it doesn’t strike me as something that should fall to the trust to have to subsidise. Echo is an increasingly utilised skill and the one that hospitals need their physiologists to be proficient in. If it isn’t being taught at undergraduate or masters level, then trusts will have to pay for the training and overtime required to bring their staff up to speed with each new generation of practitioners.
Over the summer, my university has purchased an echocardiography unit, so I assume we’ll have a bit of a head start, but surely if the practice of echocardiography is so important in the profession, it’s something that should be mandatory to teach in the academic training. Perhaps this is something that will be factored into the equation as the PTP and STP courses continue to change over time.

















 Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.
Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.