When Cardiologist’s Kitchen put forward its Health Foundation application, it stated that it would run patient workshops at Neston Park Farm & Kitchen to engage patients with professionals and good, healthy food.
Neston head chef Steve Mercer cooked a fabulous 2-course meal for guests, and after a brief interlude by Ali Khavandi and Mary Fifield, there were some indroductions for myself, nurses in Cardiac Rehabilitation and the CardioFITr team (more on these guys in the future), as well as local food producers Fussels, and Fresh Range, whose ingredients made up some of the food.
The workshop wasn’t about us, however; it was a patient-centred event, so the real stars of the evening came in the form of the service users themselves. A select few were gracious enough to share their stories regarding the improvements that Cardiologist’s Kitchen had made to their lives. One had lost a considerable amount of weight and thus, could do normal, everyday things that she had previously found difficult as a result of her (now greatly improved) angina, another was part of the CardioFITr programme, which, run by healthcare professionals and in conjunction with Cardiologist’s Kitchen, uses evidence-based science and medicine to improve physical fitness and promote a continued change in lifestyle. He too, had seen a considerable and positive reduction in weight and blood pressure, and was almost ready to cease his medication for the latter. This is a particularly palpable achievement for the scheme, and proves it actually supports patients to persevere.
A 2010 paper by Curtis Triplitt of The University of Texas titled Improving Treatment Success Rates for Type 2 Diabetes cites clinical inertia as the biggest barrier to treating the condition, so by beginning to see positive results in this manner, initiatives like this really do matter with regards to health and wellbeing. It’s long been known that diet and exercise have a massive impact on health, but anyone who’s struggled with dieting, knows that support is one of the most important factors in sticking to whatever regime one is using to better their health.
As I chatted to patients and heard their stories, I became aware of just how thankful they were for Cardiologist’s Kitchen, and the positive impact it was having on their lives. Many of them had been rushed to the Catheterization Laboratory with a suspected infarct, and regardless of the findings had assumed their lives were irrevocably altered. The advice and specific support given by CardioKit meant they were now turning a corner and seeing measurable changes in their own health. The best part was knowing that they had essentially been encouraged to do it themselves with their own willpower.
Barely a month goes by without a national newspaper displaying words like “science says _________ is bad for your health”.
Don’t get me started…
I concede that *some* of these headlines might be correct, but it’s worth taking them with a pinch of salt, if you’ll pardon the pun; firstly, “science” isn’t an all-powerful being that performs every possible study single-handedly, so it’s difficult to know exactly who has put forth the particular claim and how many people through whom the information has passed before it gets to the news media, and secondly, “science says…” doesn’t necessarily mean it’s double-blind, peer-reviewed, evidence-based or ethically funded, so between the debunked results of Andrew Wakefield’s infamous autism/ MMR study and big pharmaceutical companies potentially protecting their interests by omitting unfavourable study data, it isn’t a great idea to believe that eating bacon causes your lips to fall off, simply because the junior science editor for The Daily Expresstells you it does.
What, then, do you believe? Nobody wants to find themselves being brought into a Cath Lab, and they don’t want the uncertainty that comes with not knowing whether the food that they’re eating is going to help put them in that position. This is where Cardiologist’s Kitchen comes in; Consultant Interventional Cardiologist Ali Khavandi would rather intervene well before you’re being consented for an invasive procedure, and addresses issues with cholesterol, weight, blood pressure and diet by way of a pre-emptive strike using evidence-based dietary and lifestyle changes.
Cooking Cardiologist, Ali Khavandi
Not unlike this site, the initiative began as a humble health-based blog in 2015, featuring advice and recipes, and was borne through personal, clinical experience. Khavandi’s passion for both cardiology and cooking pushed him to create a resource, and seek a wider market using the same mechanisms employed by the media and the food industry, but using an evidenced basis in cardiovascular wellbeing. The Health Foundation has since granted the Cardiologist’s Kitchen project an award that has allowed the trial of this innovative approach to healthcare to really take off!
Currently, Cardiologist’s Kitchen has partners in GP surgeries, a restaurant and various South West England food suppliers that combine to make conduit for the project’s entire message. Despite still being in relative infancy, Cardiologist’s Kitchen has made headway, and continues to open up avenues via which to get the message out there.
Patients with new or existing high blood pressure can get a CardioKit pack at affiliated GPs. I got one to sample, which contained some money off vouchers, health advice and information about the project. In addition, The Bunch of Grapes gastropub, found in Bradford on Avon, just outside Bath, offers some menu heart-healthy menu items devised by both Ali Khavandi and head chef Steve Carss (I’ve sampled some of these too; they’re delicious).
The recipe for this Chinese chicken and more, is available on the Cardiologist’s Kitchen website
The website is the real central feature of the initiative, with healthy recipes, incentives for transforming your attitude to heart health, and evidence-based discussion on food fact, cutting through scaremongering in the bad science which can sometimes surround food.
Rather marvellously, it encourages the use of local suppliers by offering deals and home delivery on their seasonal produce. They’re also in the process of developing ready meals specifically designed to improve cardiovascular health.
By using CardioKit, the aim is to lessen the need for medication, and support local business as well as your own heart. If you’re reading this, and it applies to you as a patient, then I urge you to have a look. If you’re a practitioner, definitely do the same, and get in contact with the CardioKit team to see how you can get involved.
Inspired by the advice presented on Cardiologist’s Kitchen, I made a rather lovely Jamaican beef curry, the (really easy) recipe for which I will share here:
250g lean diced beef
4 banana shallots, thinly sliced
1 x jalapeno chili, diced. (Leave the seeds in if you’re a daredevil)
1 x carrot, peeled and chopped
1 x small sweet potato, peeled and diced
1/2 mango, diced
2 garlic cloves, sliced
1 box passata
1 tbsp. jerk paste (jerk seasoning will do fine, but add 2 tbsp.)
1tbsp garlic granules
1 tsp. tomato puree
100ml chicken stock
Greek yoghurt
Flat leaf parsley, roughly chopped
Salt and Pepper, to taste
Rice, any kind, and enough to feed 2 people
With a little oil, brown the beef until sealed sufficiently. Add the shallots, sweet potato, and sliced garlic, and cook for another few minutes. Throw in all of the other ingredients and reduce heat. Simmer for 60 mins, or until the beef is tender, and use this time to cook your rice. Serve with some chopped parsley and a dollop of yoghurt.
I recently spent the day inside the catheterisation laboratory, specifically in the pacing lab. After a few relatively straightforward implants, we reached the final case of the day; a pacemaker change. The patient in question had 4 months of reported battery life left on his pulse generator, so on paper, it was merely a case of opening the pocket in which his old device was housed, and switching it out for a new one that would stimulate his heart for the years to come.
Textbooks are great, in that they detail a procedure from start to finish, usually from everyone’s perspective, covering all bases regarding technique, equipment, potential emergencies, and possible troubleshooting options should the need arise.
These emergencies range from device malfunction to cardiac complications, and cover most things in between. I haven’t read a textbook that outlines what should be done if the patient suffers from dementia, however…
The procedure began late due to the difficulty in cannulating the individual, given they didn’t really understand where they were, and began thrashing around wildly in confusion as soon as the needle was introduced, but eventually they were brought into the lab and set up on the table. Local anaesthetic was administered whilst myself and other members of staff present tried to ensure that the patient was as calm as possible.
This proved rather difficult, as the patient was understandably scared; bright lights and masked strangers staring down at you aren’t a pleasant experience for anyone, so add a severe perception deficiency into the mix, and it’s only going to be worse.
Once the procedure proper had begun, it got so much worse.
If you’ve ever been in a lab or theatre when an electrocautery is being used, you’ll know how loud it is. Trying to keep a confused patient calm, and focussed on your voice alone, is incredibly difficult when you’re being drowned out by a deafening beeping noise. The consultant performing the change was having to work 3 times harder than normal whilst completing his task, because of the patient’s inability to understand what was happening, and more importantly, why it was happening.
There were 6 staff in the operating lab, and of those six, the only one able to fully focus on their job was the consultant. The rest of us tried to hold a limb each, to stop them from flailing and causing potential injury.
The chief priority was the patient’s overall well being, so when the radiographer received a rather nasty set of deep scratches, she endured the pain and tried to reassure the patient.
When the registrar’s fingers were being held so tightly together that they almost broke, she quietly asked if I could free them using one of my available hands, and continued talking to the patient.
When I was struck in the face as a result of removing a hand from the patient’s leg in order to do the above, I didn’t make a sound, as I didn’t want to frighten the patient anymore.
In this patient’s mind, we were causing discomfort for no reason, and as a result, this patient was fighting as though his life depended on it, but nobody said anything that might give cause to further agitate him no matter how much was thrown at them in that situation, because the fact is, we were there to help the patient and their safety came before our own.
No amount of reading could have prepared me for that situation, but even a small amount of warning, or advice, would have been a boon. To that end, I’ll say this;
Scenarios such as the above WILL happen. It’s inevitable. Just stay calm, communicate with everyone around you and never forget why you’re there. Of course it’s not right that you sustain an injury on the job, but the bigger picture comes first and then you can set about producing system changes.
I must have walked past this building thousands of times over the years. I’d always admired its exterior, whose 18th century aesthetic still fits perfectly with the rest of Bath’s modernised Georgian motif. The stonework might be slightly mottled and tarnished by years of pollution, and its being surrounded by coffee shops and high-end clothing outlets *almost* detracts from the majesty the building exudes, but the Royal National Hospital for Rheumatic Diseases, nestled right in the North Somerset city’s centre still looks beautiful. I remember the public outcry when it was announced that a large chunk of the building had been sold, and subsequently leased to a novelty Mexican food chain; this building is a part of this city, not just for the patients treated within it, but for all of the residents of Bath.
Despite admiring it from the outside, I’d never consciously considered its interior. I’m not sure how many people actually have, to be honest; those I questioned had either never looked past the front doors, or had simply “heard it was quite nice” through the grapevine. I recently had the opportunity to begin to learn echocardiography at the RNHRD in Bath, and whilst I was waiting for my superiors to arrive I decided to have a look around, as it was clear from stepping through the front doors that it was a building steeped in history.
The main foyer is rather breathtaking: the original marble floors are still a prominent feature just past the reception area, paintings, such as that which is the header on this article adorn the walls and connecting the ground and first floors are beautiful, finished wood staircases that look like something out of Disney castle. I had to stop for a moment just to take it all in. Having spent a fair amount of time in hospitals, I had assumed that they (for all intents and purposes) look pretty similar; white walls, long corridors with small, commissioned pieces of generic mixed media/ abstract work hung at eye level along them, and that style of lino flooring that evokes memories of the school gymnasium, squeaking underfoot at the slightest hint of moisture on one’s shoes. Now, I’m not saying this is a bad thing (far from it), but the RNHRD has a unique character. It has charm and detail that I’ve only found in stately homes and upscale galleries. It also has history to rival these places.
Frances MacDonald, 1949
The funding for the hospital was procured predominantly via a public subscription set up by Richard (Beau) Nash in 1732. Names such as Lord Palmerston, Mr Jeremiah Pierce, and Dr William Oliver are listed as donors, as well as other local and national figures, and as a result of their capital, the building, constructed as a hospital for the sick poor opened in 1742. Built using stone gifted by local legend Ralph Allen, the then Bath General Infirmary was the first hospital to offer treatment to the entire UK, leading many to view it as a foundation of the National Health Service devised in 1948.
Locals, or those fond of UK trivia will likely already be aware of the hot springs on which Bath sits, and these were utilised in the hospital for therapeutic purposes (interestingly, Bathonians were, for a time at least, not permitted to become patients of the Infirmary, presumably because they as residents, already had a right of access to the spring waters), and these were made available to patients on condition that a fee be paid upon admission. For English patients, this was around £1.50, which later became £3, and for those from Scotland and Ireland, £3, which became £5. These sums were either paid for by the patients themselves, or on their behalf by wealthy benefactors, and covered the cost of treatment and the return home, or, in the worst case, mortality and the subsequent burial arrangements.
Patient sedan chair
A brass badge, worn by a patient whilst under hospital care
Patients were taken to the bath sites via hospital sedan chairs (designed by surgeon Archibald Cleland, subsequently dismissed for improper conduct in 1743), and impelled to wear brass badges that both identified the patient number and their ward, and to prevent drunkenness whilst out of the hospital grounds. Local landlords were forbidden from serving alcohol to patients, as it was detrimental to their recovery. Failure to adhere to this rule would have risked their licence, so it was likely seldom flouted.
The hospital was initially far smaller than its current size, with new wings and blocks being added throughout the years, including the top floor in 1793 (costing £900), renovation efforts and the implementation of additional units continuing well into the tail-end of the last century.
The Roman pavement, discovered in 1859
When the building was being extended in the late 1850’s, a Roman pavement was discovered during the foundation digging. It is dated as hailing from between AD60 and AD410 and is still in place at the bottom of the stairs to the basement level. The mosaic is still part of a larger floor and runs underneath much of the building itself.
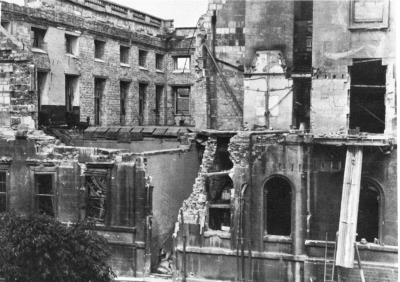
Given the tenure of the building within the city, it has seen its fair share of conflict; as well as being used to treat the wounded during the Jacobite Rebellion, the Crimean War, South African War and both World Wars I and II, it suffered damage due to ordinance during the latter conflict in 1942 wherein it received a direct hit. Despite this, however, the roughly 200 patients still within the confines of the hospital were uninjured.
Damage to the RNHRD in 1942
As far as treatment goes, the hospital has been a specialist rheumatology centre since it opened, and continues to operate as such. It offers treatments for pain management, chronic fatigue and utilises hydrotherapy as it did when it was concieved. It also functions as a research centre in these areas, encompassing both in-house studies and those of a more national variety. In addition, and I feel rather interestingly given its history with servicepersons, the centre offers specialist support to ex-military personnel, regardless of the time of onset of condition, and provides pain-management and post amputation complication therapy amongst other things.
Royal Patrons have presided over the RNHRD since its foundation, with the current President being Camilla, Duchess of Cornwall, who has been in the position since 2006. The first, in 1745, was Frederick, Prince of Wales. In 1991, the RNHRD became an NHS Trust, and was upgraded to an NHS Foundation Trust in 2005. In February 2015, the hospital was acquired by the Royal United Hospital (RUH), Bath, which now manage the centre.
The Royal National Hospital for Rheumatic Diseases truly is a wonderful hospital, and the patients who use its services do so over a number of years, crediting it with a “family feel”. Whilst researching this article, I spoke to a volunteer at the hospital, who told me of her time as a patient, both in and out, and her desire to provide a friendly ear to current service users. She told me that volunteers had relaxed her when she herself needed the hospital’s facilities, and it was that, combined with the care she was provided that inspired her to give back to the trust.
The family feel of the RNHRD was in jeopardy whilst the hospital was under considerable financial strain, but its acquisition by the RUH allowed it to continue to function with only minimal service absorption by the Royal United. This continued service will surely help the current patient base, and will enable the hospital to remain the part of the city that it has been since its conception.
This flag hangs over the museum, and was made to celebrate the 250th anniversary of the RNHRD.
Rather wonderfully, the hospital contains a museum, situated in the chapel, which outlines the history of the building and the staff and patients who have used it throughout the years. Many of the photographs found in this article were taken in the museum, and it’s full of information about the building and its history; well worth a visit if you’re in the area!
Thanks to the museum staff at the RNHRD for taking the time to talk to me and allow me to take photographs. Without them, I wouldn’t have been able to write this article.
If you’re eager to explore more, head over to Medical Heritage or visit the RNHRD homepage, and if you’re local to Bath, then be sure to drop into the Bath Medical Museum, situated within the RNHRD.
Myself and OliGS recently sat the SCST Electrocardiography Diploma and Practical Examination, so I thought I’d jot down some of my experiences in the run up, and my retrospective thoughts on the day itself.
If you’re thinking of doing it, or have your PTP finals looming, then read on, as this will give you an idea of what to expect.
I’ll start by saying this: Oli and I have NEVER been so stressed in our entire lives.
This exam was a nightmare for which to prepare; I have extensive experience in taking exams, and it is my view that they’re 50% what you know, and 50% what the examiners want you to tell them. Without having met these examiners or seen a previous paper, it was very difficult to know what to really nail, in the revision stage. The syllabus was long, detailed, and contained what seemed like an entire career’s-worth of things to learn, so we already knew it was going to be a slog, but nothing prepared us for the written paper…
Read these. Lots.
We studied, sometimes sleeplessly, for weeks. Tested each other on rare arrhythmias, read textbooks cover-to-cover (repeatedly), and watched each other’s once sunny outlooks and youthful (ahem) features rapidly wither as the examination date draw closer. It consisted of 20 multiple choice questions, 10 arrhythmia analysis and knowledge questions, and 4 full ECG analysis recordings. Some of these were almost instantly recognisable, but others were brutally difficult to analyse. The MCQs (often the most looked-forward to section of any exam) were equally tough. Those 3 hours lasted a lifetime…
We left the exam battered and bruised, but glad it was over.
But it wasn’t over. It was far from over. As well as the written paper that had almost ruined us, we had the practical exam to do as well.
We had made sure that during our post-ECG placements we still got ourselves in the clinic so as to keep everything fresh, as performing a perfect ECG is not like riding a bicycle.
The last attempt before test day
It turns out that this was the correct call, as was practicing on one another in the hotel the evening before the exam; the margin for error in the exam is 2mm(!) Anyone who’s had an informal assessment, or had their Direct Observed Practice scrutinised whilst training knows that it’s very easy to second-guess when it comes to electrode placement, and despite having 20 minutes to complete the whole thing, this timeframe becomes devastatingly short once you’re in there. It’s a clinical assessment, so one needs to complete the necessary ID checks, explain the procedure to the patient AND to the examiners (i.e. in two different ways), perform it whist answering questions, and then complete a verbal examination.
Three hours after we had finished the written paper, we were called to attempt our practical exam. There were ashen faces all around. Some were on those still waiting for their number to be called as ours had just been, others had been told that their 2 attempts had been unsuccessful. Neither of us were looking forward to this. Now, given that I’ve already stated that each electrode is allowed to deviate only 2mm from the precise, gold standard location, the internet-purchased electrodes pictured in the above image would be somewhat unfair, right? It seems that the examination board concur, as they provide some rather cool, transparent electrodes complete with crosshairs. They doesn’t make it easier, per se, but they certainly go some way eliminate that lingering trepidation when it comes to deciding you’re happy with your placement and ready for judgement.
Crosshair emblazoned electrodes(!)
I opted for the “all at once” technique: I explained everything to the patient before I started, gained consent, then explained everything I was doing as I went along. Once was put simply to the patient, then once to the examiners, using correct terminology. I paid extra special attention to V1, V2 and V4, as my patient had a particularly wide sternum, so I wanted to be totally sure that I had the sternal border, especially given the electrodes were rather far apart when placed and looked slightly odd to me. After I took a step back and looked at my work, I was incredibly tempted to move the aforementioned electrodes, but either due to fear, fatigue, or a combination of the two, I decided to leave them as they were, opting to go with my initial judgement. After that, I waited.
I’m not entirely sure how the placements are measured, as candidates are asked to leave the room whilst they are checked by two examiners. I heard someone mentioning special rulers, but I didn’t get a look at them (it’s all very cloak and dagger), in any event, you’re called back into the room and, in my case at least, informed of your passing or failing grade. I’m pleased to report that I passed on the first attempt, which as I’m sure you can imagine, was a tremendous relief; I lost my cool somewhat, and expressed my joy rather loudly, as I was informed I wouldn’t have to do it again. Oli soon found me in the waiting area and, grinning wildly, slapped me on the back and hissed “YESSSSS!” before promptly throwing himself into a chair. It was over, and we were victorious.
We didn’t speak too much about it, on the way home, but in the couple of days that have passed since the exam, we both feel a tremendous sense of pride that we actually did it, and did it successfully. If I were to give you all some advice, it would be the following:
Be prepared for anything and everything, including waiting around for a long while
Practice analysing ECGs until you hate them
Practice performing ECGs until you hate them
Go with your gut as much as you can during the practical exam
Bring lunch
Don’t under ANY circumstances, stay at the Ibis Hotel in Birmingham’s Chinatown district (I can’t stress this enough because it backs onto a nightclub that doesn’t stop playing the most bass-heavy music until the wee hours of the morning)
A cardiology fellowship will give you the opportunity to be fully prepared for the field and can go as long as four years. It will help you to hone your clinical skills and have cutting edge skills in surgery. A mix of research, public lectures, clinical experience, and classroom-based learning all combined enable one to be very well versed in the field at hand. Fellowships in Cardiology range from Cardiac Surgery Training, Cardiac Critical Care and Paediatric Cardiology, Vascular and Interventional Radiology, and Vascular Surgery and Endovascular Therapy Fellowships.
Several institutions offer what are considered the best Cardiology Fellowship Programs. To choose and get accepted into the best cardiology fellowships programs successfully, requires much more than an exceptional personal statement; applying to a residency, especially a cardiology one, is challenging and requires a lot of work. The existing places for such mentorships are extremely limited and contested, so you have an obligation to be unique and to stand out in order to be accepted.
Your cardiology fellowship personal statement is an opportunity whereby you can say why you feel you are the most deserving of being enrolled in the program. Elevating yourself above the bar will determine whether you are accepted or rejected. Here you will find the help to writing a personal statement for fellowship in cardiology, as well as some dos and don’ts.
Fellowship goes above and beyond a good resume. A good resume can only go a long way. You can be the most qualified and have the best CV, but this will not guarantee you a spot in the fellowship program. As a candidate, do research on your options, enhance your exposure on volunteer work, conduct clinical research projects, and get publications. Ensure that you have filled the gaps in your resume and took the time to address all of them practically. Most candidates limit their options depending on where the hospitals are situated. This approach is detrimental, however, and prevents them from having a varied list and therefore options pertaining to the top-notch institutions. As a candidate, you can polish up your resume with a clearly defined and well put together personal statement.
The AMA or the American College of Physicians. Most candidates are not part of any corporate entity that advocates for their medical practice. With the continuous cutting of funds in the national budget, it is getting harder and harder to provide any services. This, in turn, has reduced the number of applicants able to be accepted and therefore numerous candidates find themselves being turned down. Joining the AMA will help you get a fair trial and increase your chances of getting approved.
Application to highly competent residency. Programs in radiology, dermatology and cardiology are highly competitive, and the stakes are high. Some of these students’ performances in their former medical school are usually not up to standard and sometimes place few schools on their ranking list.
Expansion of classification list. Students tend to limit their options and apply to a few residency programs. However, it is encouraged that a student lists down at least five hospitals to increase their chances of getting accepted. These choices can either be within their chosen specialty or even selecting a different specialty.
Transitional slot. A student can contact their medical school and ask for an interim slot or see a research fellowship. With this, the candidate will be able to become more competitive in the field and increase their chances of approval. An additional degree is also a supplement to a candidate’s resume and consideration.
Ill-preparedness. Two or more years of postdoctoral training whereby there is formal coursework in the fundamental sciences pertinent to the investigator’s area of expertise; this increased chances of attaining a fellowship.
Medical residency interview. It’s like a pass mark for all residents. Most programs won’t absorb candidates they have not interviewed. It is crucial that you take this interview seriously as it will not only determine if you will get accepted but also where you will get accepted.
Robin Dale is a junior doctor and her passion is guest post writing. She is fond of writing useful posts for students to make their learning lives easier and more effective. Her own life credo is “Keep calm, study hard, and become a doctor”.
EDIT: The Android version of TSP Mobile: ECG is available for download, but due to the way in which Google Play operates, I have been unable to offer it for free. The iOS version, when available, will be gratis for the promised 14 days however. Still no word from Apple when that will be, but I have been assured that it is being vetted as I type this, so fingers crossed!
Original article follows:
Well, that TSP mobile app I promised…
I’ve been saying I’d do it for months and, despite remaining fairly quiet with information about starting, I actually have been working on it. So much so, in fact, that the bulk of the development is finished! It’s in final stages of testing, after which it will be available on the Google Play and iOS app stores, where it will be free for the first two weeks of release, so please download it and leave some constructive feedback and a review.
The app features tutorials on ECG analysis, exercise and ambulatory ECG, cardiac flow and cycles, action potentials and useful formulae for trace analysis. Each section is laid out in an easy to follow format, with colourful diagrams and both real and illustrated ECG traces.
Heart rate and QTc calculators are included to aid analysis without leaving the app, and also access to the website blog, so you need never miss an update.
This slideshow requires JavaScript.
I hate advertisements in apps, so in order to keep TSP mobile ad-free, I will charge £1 to download it after these introductory 14 days are over. In an ideal scenario, I would keep it completely free, but it has been, and continues to be, a rather expensive endeavour from both a chronological and economical standpoint especially for my shallow, student pockets, so I hope you understand why I have decided to charge.
Stay tuned to TSP via site, Twitter or email for a release date. It’s very soon!
On the 24th of September, the BBC reported the story Nina Adamowicz. Nina, a 72 year old lady with an Implantable Pulse Generator (IPG) who, after having the device for almost 20 years, has requested it be switched off.
After suffering a minor infarct, Adamowicz had said that her continued deteriorating health became too much to bear, said she felt like she was waiting in line to be executed, so she requested her device be switched off. She is reported as stating “It isn’t about ‘I want to die’; I’m dying”.
Her case was referred to her local trust’s ethics committee, who, after careful deliberation decided to proceed in line with the wishes of Mrs Adamowicz.
Before passing away on the same night that her device was switched off, Nina Adamowicz stated that she believed she had the right to decide whether or not she wanted the IPG on or off, and stood by her decision.
This case is thought to be the first of its kind in the UK, but Chicago device specialist Dr Westby Fisher professes to doing this exact thing on a dozen separate occasions. Westby considers the ceased action of an implantable device to removing a feeding tube, or switching off a ventilator.
In particular, in a piece for massdevice.com, Fisher tells of a patient who refused dialysis, saying he’d rather let nature take its course. The patient, who also had an IPG, requested that this was switched off, so Westby agreed, and the next day switched off tachyarrhythmia detection on the device. Fisher says that he feels that both he and his patient did the right thing, together.
I for one, am confused as to the ethical pathway involved in coming to both this decision, and that of the ethics committee associated with Nina Adamowicz.. Assisted suicide is complex, but with respect to these scenarios, is defined as the intentional encouragement or assistance to a patient in ending their own life and it is still illegal under the 1961 Suicide Act of UK law . A medic who administers an overdose of muscle relaxants to a patient whose condition is diagnosed as being terminal, even at the behest of that patient, would be punishable by UK law with manslaughter or murder and potentially serve the maximum terms associated with each.
Why then, is hitting the off switch on a pacemaker not considered to be comparable to the example given previously? Patients with implantable devices often have them to combat life-threatening arrhythmias, so in turning them off, this can effectively issue a death sentence to that patient. I’m not arguing for or against any form of assisted death; I neither understand its intricacies or feel it is my place to denounce or advocate something with which I have had precisely zero experience, I’m simply confused as to why an immediate form of assisted dying is outlawed, and something so similar (on the surface at least), is not. Adamowicz’ clinician has said that other professionals are split in their opinion on his decision, with some feeling it to be “uncomfortably close to euthanasia”.
Is it fair to patients with terminal diagnoses that are forced to travel to countries such as Switzerland, wherein some forms of euthanasia are legal, simply because they do not have an IPG? Does the severity of the condition have any part to play? How similar do individual cases have to be so as to render one illegal and another not so? I have a feeling that this case will spark long debate throughout the medical and legal professions in the UK, and will follow its progress closely.
After my review of the temporary access trial of Epicardio Simulation (which offered a great deal of praise, I might add) I couldn’t wait to have a look at the full version’s features. I still can’t afford it yet even with the 60% discount offered to full-time students, but thankfully, the good people at Epicardio.Ltd allowed me to access the complete package so that I could review it. As I’ve already covered some of the functions of the program, I won’t re-tread old ground, but you can check out what I thought of the trial version here, and consider this a continuation of those original opinions.
So, what functionality is offered by the full version? Let’s go over it now.
The previously-unavailable tutorial section has some marvellous interactive elements; a view of the electrical action and a live ECG accompany the written tutorial pages, allowing the user to view the very thing they’re reading about in real-time. The procedurally generated ECGs are very accurate (I’ve measured them), but if you want to see a genuine patient-obtained trace recording, then one is included with each arrhythmia, too, which really helps with comparisons to the actual recordings one is likely to find in practice.
Almost everything you can think of is covered in some capacity, both on its own, and linked with other, relevant arrhythmias, so you really get a feel for just how interwoven some conduction and rhythm abnormalities can be.
A marvellous inclusion is the level of interactivity within the tutorials; degradation from VT to VF, for instance, is displayed live on the ECG strip and the defibrillator (that I didn’t really have cause to use in the trial version) can be charged, and a shock administered, altering the rhythm strip as it would a real patient.
The pacing tutorials are easy to use and easy to follow; they walk you through the physics of single and dual chamber, as well as biventricular pacing. In using them to learn the basics of pacing, I can appreciate how effective the arrhythmia sections are and how useful they would have been during the early days of my studies. The interactivity of the aformentioned tutorials remains, too. Placing a pacing wire in different sites allows the user to view live rhythm changes, and sensitivity, HR and pacing rate can be toyed with so as to identify intrinsic rates and pre-pacemaker abnormalities such as 3rd° AV Block on the real-time trace.
The test area throws generated ECGs at the student, and offers multiple answers from which to choose. Much like any degree-worthy multiple choice test, they range from incredibly easy to downright tricky, but a review section allows you to view the areas that might require further learning before each future run-through. As with the main bulk of the software, measurement calipers are useable during the test, allowing for some precise questions to be given. Importantly, this software allows and encourages repetition; fundamental to successful learning. It may seem obvious, but I noticed that my understanding of unfamiliar areas increased the more I explored them. What won’t be obvious, is just how quickly this occurred. With the addition of the test function, the user can consolidate what they have learned at their own pace, and not have to exit the program find a different testing app.
My time with the trial version of Epicardio only threw up a couple of minor issues. Whilst these are still present, they detract from the simulator even less than before, due to the myriad of extra content present in the full release. My only new problem came in the single chamber pacing tutorial, wherein I was instructed to reduce the pacing rate to 45bpm, yet I couldn’t lower it past 50bpm. This made it impossible to view the intrinsic rhythm of the digital patient (the point of the page in question’s existence), but only in this instance. It’s worth pointing out that regular updates exist to iron out glitches such as this, so errors needn’t remain for long.
If, like me, your learing speed is increased by doing, as oppose to just reading or seeing, then you’ll find this tool invaluable. To be able to safely induce life-threatening ventricular rhythm is, understandably, an uncommon occurrence, so a method to facilitate this, and things like it, is always going to be welcome for students. In Epicardio, however, you get so much more than that. Pacing of all types is covered in depth, real and digitally created ECGs, and an effective test facility really do set this above any of the other programs that I’ve used. It’s also incredibly simple to get the hang of, too. The things it does well far outweigh its minor issues, so I can wholeheartedly recommend this program to everyone who wants learn about cardiac arrhythmia and interventions. Whilst the implementation of a 60% student discount brings the price down to the £59-£89 mark, it is still expensive, but you really do get what you pay for.
Recently, in a Holter clinic, I dealt with an 8 year old patient who was on the road to recovery after a diagnosis of congenital defect, Tetralogy of Fallot. As a result, I got hold of the most interesting ECG I have recorded to date.
Background
ToF is a rare congential defect affecting the heart, that results in an insufficiency of oxygenated blood leaving the heart through the systemic circulation. Thus, it is considered a cyanotic disorder.
The disorder affects roughly 5 in 10,000 infants, and has an equal gender distribution.
Generally, four pathologies comprise ToF. Whilst all four are not always present, three can consistently be found. ToF is a progressive disorder, in that each pathology gives rise to the others.
Hole in septum, due to malformation, causing oxygenated and deoxygenated blood to mix within cardiac structure
Overriding Aorta
Aorta is placed over VSD, transporting blood with low O2 content to wider systemic circulation
Cyanotic episodes require immediate correction, before surgical intervention.
High flow O2 administration
Physical positioning
Knees to chest
Parent cradling the child will illicit this effect naturally
NaCl fluid bolus
Vasopressor therapy
Increases systemic vascular resistance, shunting blood through pulmonary system.
Continuous ECG and SpO2 monitoring
Surgical intervention usually repairs the VSD and addresses pulmonary pathology, often at the same time.
Prognosis for ToF patients is generally very good.
Overall outcome improved since surgical treatment has improved
Survival of surgery is currently 95-99%
36 year post-surgical survival is currently 96%
Patients who undergo surgical treatment are at greater lifelong risk of ventricular arrhythmia
Complications can arise as a result of a transannular patch repair, specifically;
RV dysfunction
Heart block (risk of HB has dropped to around 1%, in recent studies)
Heart failure
Recurrent or residual VSD
Hx:
8 y/o
Previous diagnosis of ToF
VSD
PV Stenosis
Mild RVH
Treatment:
Transannular patch repair
PV Replacement
Medication:
Daily:
Atenolol
Aspirin
This patient was having a 24hr Holter recording to assess cardiac recovery after their most recent procedure; the PV replacement. Physical examination showed a RVOT murmur, whilst echocadiography displayed a mild RVH and PV regurgitation. Left heart functionality has been classed as excellent.
Previous ambulatory study has shown no arrhythmic action, save for that considered normal in a child of this age. No previous ECG recordings were available.
Upon monitor removal, a 12-Lead ECG was performed, the resulting trace was as follows:
Ambulatory analysis relating to the most recent study did not differ greatly from previous monitoring, showing occasional sinus arrhythmia and bradycardia, five non-conducted P waves were found, and two of these gave rise to periods of sinus bradycardia. All other instances were gradual onset/offset.
Nocturnal bradycardia reached rates as low as 34bpm.
What does everyone think of this ECG and brief ambulatory report? Let us know by leaving a comment below!