Scouring the web for cheap textbooks, I happened upon something of which I wasn’t even remotely aware: alternate ECG lead placements. As has been highlighted in previous posts by myself and others, cardiac scientists have strict guidelines that ensure we perform an ECG procedure to an accurate and repeatable standard, so it came as a bit of a surprise to discover that there existed a different way of carrying out the test with an aim to view specific activity.
The Lewis lead, named after Sir Thomas Lewis, is an alternate placement that can be used to better view atrial activity in relation to that of the ventricles. In many ECGs, it can be rather difficult to assess P waves; whilst they are represented using standard lead configuration, they are much less apparent than ventricular activity, due to the nature of the ECG’s detection mechanisms.
Using the Lewis lead configuration, it is possible to increase the detection of atrial activity and diminish that of the ventricles and gain a clearer picture of atrial fibrillation, flutter and, in the case of the article that brought my attention to this system, improving P wave recognition in wide QRS complex tachycardia.
The configuration is as follows:
RA electrode on the manubrium
LA electrode on the 5th IC space, right sternal border
LL on the right lower coastal margin
RL remains in the standard SCST position
Adjust calibration to 20mm/mV
As shown on the diagram, a three lead configuration is still present, as in Einthoven’s triangle, but Lead I now travels directly over atrial activity. For this reason, Lead I is used as the monitor lead and the one from which a rhythm strip should be taken.
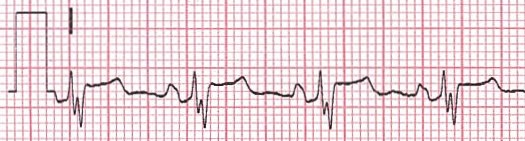
On the trace itself, there is a marked visual difference. The following were recorder on the same patient and we begin with the standard electrode configuration:
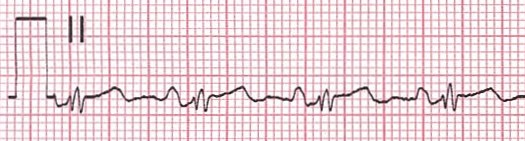
And now introducing the Lewis lead setup:
The P waves present in these altered leads are much more pronounced.
There are more lead systems that are used in the diagnosis a variety of different conditions such as Brugada syndrome. I’ll research and cover these and try to get some more traces using the Lewis lead system throughout the year.
As a student cardiac physiologist it has been drilled into our heads from an early stage the importance of correct anatomical electrode placement in obtaining an accurate ECG recording. An ECG measures the electrical activity of a patient’s heart from many different angles, and is achieved by placing 10 sticky electrodes on the patient; four on the limbs and six on the chest. For correct electrode placement we follow the clinical body guidelines set out by the our governing body, the SCST. As specialists within the field, we have a duty to perform these tests in a standardised, methodical manner to produce reliable and accurate diagnostic information, as the ECG is the first port of call when assessing heart abnormality.
Unfortunately, from my experience, and from that of my colleagues, the misplacement of these electrodes has become somewhat commonplace. To the unassuming operator this may seem superficial but incorrect placement of electrodes can alter the ECG patterns displayed simulating or concealing abnormalities, such as myocardial ischemia/infarction.
There is evidence that many health professionals who record ECG’s have not been suitably trained or assessed in the technique: A study by Kings College London into electrode misplacement highlighted that only 50% of nurses and less than 20% of cardiologists correctly place leads V1 and V2 during a standard 12-lead ECG. These numbers are quite shocking and highlight the widespread misunderstanding of this key diagnostic tool.
An example of how NOT to perform an ECG. V1 and 2 are incorrectly placed, as are 3 and 5.
I personally witnessed an example of this whilst on my first week of placement. I was performing an ECG on a patient within the cardiac ward under the supervision of an assistant technical officer who regularly performs ECGs. I correctly located the anatomical landmarks on the patient’s chest and applied the electrodes, as per the official guidelines. At this point, the ATO interrupted me and challenged the placement of my V1+V2 electrodes, stating they were too low. She then took over control of the procedure and removed the electrodes. She began to count the intercostal spaces, beginning from the clavicle. The guidelines state the operator should identify the manubriosternal joint, or angle of Louis, on the patient to locate the second intercostal space as their first anatomical landmark. This subsequently meant her V1 and V2 electrodes were placed too high and my original placement was in fact correct. After the procedure I challenged my colleague about this explaining we were taught to follow the SCST guidelines in our electrode placement. The ATO responded by saying that this was “how they had always done it.” I discussed this with my clinical educator and the issue was later addressed with my colleague.
The consequence of incorrect ECG recording can lead to potentially incorrect diagnoses and inappropriate treatment leading to wasteful use of healthcare resources and even cause harm to patients. Evidence suggests that adequate training of operators reduces ECG recording errors. However as the SCST highlights in their guidelines, the indications there is little awareness in many practitioners of the need for training.
Clearly, the solution to this issue is to increase awareness in health professionals exposed to ECG practice about the importance of correct electrode placement. This could be achieved by increased collaboration between cardiac physiologists and other healthcare professionals. As specialists within the field we have duty to share our expertise and knowledge to ensure our patients receive the best standard of care. As a profession we should be much more active in teaching and increasing awareness of what we do and why it is so important. Relevant staff should be confident in performing ECGs not because of experience, but due to high quality training and continual auditing.
To achieve this I feel our profession needs to embrace this responsibility and be far more active in the support and training of other health professionals.
Khunti, K. (2013) Accurate interpretation of the 12-lead ECG electrode placement: A systematic review. Health education journal . 73 (5) pp. 610-623.
Harrigan, H., Chan, TC., Brady, JW. (2012) Electrocardiographic Electrode Misplacement, Misconnection, and Artifact. The Journal of Emergency Medicine [online]. 43 (6), pp. 1038–1044.
“Cardiac failure is a critical condition that results in life-threatening consequences. Due to a limited number of organ donors, tissue engineering has emerged to generate functional tissue constructs and provide an alternative means to repair and regenerate damaged heart tissues.”
Such is the sentiment from Ali Khademhosseini and a team from Massachusetts. In fact, they reported here, that in 2009 an average of 77 U.S. citizens underwent transplant each day, but 20 died as a result of a lack of organ availability. The aim, then, in the absence of treatment, is to repair the damaged organ in-situ so as to negate the need for transplant at all.
Enter hydrogels.
Hydrogels are already used in the regeneration of a variety of tissues, and combined with some of the brightest minds in the field significant advances are being made in regenerative medicine: in May this year a team in Toronto have successfully repaired brain tissue after stroke and partially reversed blindness. These versatile substances are also used in disposable nappies, silica gel and contact lenses, so there’s a high chance you’ve already been exposed to them without even knowing it!
These polymers exhibit many desirable characteristics in regenerative medicine. They are relatively easy to synthesise, they can act as solute transports/drug-delivery systems, exhibit elastic properties as well as preventing thrombosis. Their structure also enables them to create a “scaffolding” for cells.
This last point is crucial when combined with the hydrogel’s other properties, but I’ll return to that shortly.
First, consider what happens to cardiac tissue after an acute myocardial infarction: during infarct, the oxygen supply to myocardial cells is reduced or diminished, causing irreversible cell death and necrosis around the occluded artery/arteries. The scar tissue that takes the place of the once-functioning cardiac muscle has none of its contractility and the heart is far less efficient as it once was. Cardiac output, systolic and diastolic functions are affected and whilst medication, reperfusion techniques a bit of luck regarding preserved left ventricle function all provide a better prognosis, heart failure is a serious risk and figures regarding mortality rates aren’t great: MI, specifically STEMI brings with it a 30% mortality rate, 50% of this figure dying before hospital admittance and 10-15% being re-hospitalised one year after the index event.
So, where do hydrogels come into the picture?
In the case of extreme loss of cardiac function and the inability of conventional treatment to improve the given prognosis, hydrogels provide an environment in which it is possible to introduce stem cells, growth factor, gene injection or therapeutic medication in an ‘artificial’ environment that simultaneously provides mechanical support to the infarcted area and aids in the replacement of necrotic tissue. As well as being a relatively non-invasive procedure when it comes to the injection of the treatment, the hydrogels scaffold itself is naturally degraded by the body when the process is complete.
According to another team in Massachusetts, published here, trials have shown significant success since they began in small animals, but their application isn’t as straightforward in large primates. They commenced in humans in 2008 (in an extremely truncated form), but in order for hydrogels to be viable in widespread clinical treatment, much more research is required. An example of this is that not much is known about the exchange of signals that take part in the movement of stem cells to an injured myocardial tissue post-hydrogel treatment. Optimum degradation time is a further issue in humans.
Despite these, and other setbacks, there remains great promise in hydrogels to lower global mortality rates as a result of MI. In recent years, significant advances in research are making the possibility of myocardial repair in humans an almost visible reality.
The Athletic Heart Syndrome isn’t indicative of any pathology in athletes, and although it is theorised that the changes the heart undergoes as a result of training, there exists no evidence of long-term effects. The athletic heart often has a resting rate much slower than that of an individual of a less active nature. This is not uncommon in physical athletes, as it has been reported that Sir Chris Hoy has a resting HR of 30bpm and fellow cyclist Miguel Indurain one of just 28..!
The cause of this is a very active vagal tone, resulting in bradycardia. As I’m certain many of you are aware, this is a condition that would almost certainly (correct me if I’m wrong) require pacemaker intervention in elderly patients, but in the case of athletes, this bradycardia is due to an increased stroke volume which means the required workload of the heart is decreased. All well and good whilst one is in training, but what if this lower HR did not ‘reset’ to within the normal parameters once training had ceased? I don’t think I’m incorrect in assuming that this would lead to the same treatment a non-athlete, former or otherwise, would receive anyway, regardless of any prior level of fitness.
There is in fact a 2007 study by Baldesberger et al, that suggests this is indeed the case.
Published in the European Heart Journal and found in full here: http://eurheartj.oxfordjournals.org/content/29/1/71 it is shown that there is a statistically significant increase of sinus node disease in the tested former cyclists when compared to the control group, in this case golfers.
Interestingly, I have stumbled across a British Heart Foundation- funded study run in part by the University of Manchester, that they feel suggests the increased presence of arrhythmias in athletes is due to molecular changes as oppose to increased activity in the autonomic nervous system.
The study in rodents showed a decrease in HCN4, a protein found in the mammalian SA node. In humans, a mutation in the HCN4 gene is sometimes found in patients exhibiting sick sinus syndrome and in those who display bradycardia, so the teams behind this study believe that if they can replicate the rodent’s results in humans, it will help us understand arrhythmias that endurance athletes often suffer in later life.
I’ll answer my second question, “if so, what is the cause?” with an obligatory “je ne sais pas”, but it’s clear that we are edging ever- closer to an answer. Of course, whether that answer is due to molecular changes, or nervous ones remains to be seen.
Either way, it is stated by the team at the University of Manchester that although endurance training can have harmful effects on the heart, these effects are more than outweighed by the benefits.
As an added bonus, here is a short video by Sarah Pratt showing some common differences in an athlete’s ECG (in this case the featured athlete is the NHL’s Tobi Rieder *!*) compared with that of the rest of us. Enjoy!
As ever, if I’ve missed anything, or am just plain wrong about any part of this piece, sound off in the comments below and I’ll do my best to rectify this.
I have, however, BEEN the robot in question, as today, I provided the voice and cardiac controls in my university’s simulation suite.
My peers performed ECGs on a rather frightening, dead-eyed humanoid that was, unbeknownst to them and in conjunction with my voice, being used as a conduit for a scenario pertinent to our learning. That’s me on the right, there, next to my control station (a closer view makes up the header for this post) which allowed me to alter heart rate, breathing rate, create a whole host of arrhythmias and not only see my colleagues, but speak to and hear them as well.
I was a patient named Christopher Smith who had been admitted to A&E. That was all the information that had been supplied, barring my NHS number and date of birth. It was the job of my fellow students to check three patient identifiers, get a brief idea of what was wrong with me and to perform an ECG accordingly, with a brief assessment of the adjustments needed and that of the trace itself.
It was made clear both before and after the session, that it was ok to make mistakes and that this was predominantly what the session was for. It’s extremely unnerving, having a conversation with an expressionless robot that can visibly and audibly breathe, so it was nice to be reassured that the pressure wasn’t as high as it could have been.
Everything going to plan, it would emerge that my chest pain was a result of atrial fibrillation and a heart rate of a mere 32-35bpm. It was also an assessment of how quickly we prioritised the test itself. Due to the presenting chest pains, attaching the limb leads first, so as to gain a visible rhythm strip before a full 12-lead was the correct response, then adjusting the paper speed on the trace itself so as to provide an useable ECG was the next desired step. All the while, I was talking to the student practitioner, asking questions about the test and about the situation in order to see how they reacted and whether they felt comfortable keeping me, as a patient, calm at the same time as carrying out the test with the required level of haste.
These sessions were filmed and then followed a group feedback discussion. The group seemed pleased with the outcome, overall. The comments made were mostly of a positive nature, and the few criticisms there were from myself, my peers and our lecturer, were minor and constructive. This has most certainly been my most enjoyable session to date, and one I did not mind getting up at 4:30am to help set up, so needless to say, I’m very much looking forward to the next one.
I will add that the first half of the session used me as a living mannequin. The reasons that I didn’t comment on this until now are twofold;
It was effectively the same as what I have written about, only without the technology
Seeing my naked torso on film reminded me that I’m still carrying holiday weight. This wouldn’t be a problem, were it not the weight from four holidays.
It seems that as soon as I mentioned just how quickly this profession is evolving, something has been raised that enables me to give you an idea of how much.
This blog is called The Student Physiologist. The career’s professionals are known as physiologists or physiological scientists, ergo, myself and my peers are subsequently coined physiology students.
This, however, will soon be a thing of the past, as by the time I qualify, these terms will no longer exist. In their place will be Healthcare Scientist.
It’s difficult to find any sort of identity in such a changing professional environment and this difficulty is bolstered when a physiological scientist tries to explain their role within the NHS. We are among the most patient-facing scientists in the clinical setting, yet we are arguably the least “seen”, in that no matter the description of who you are and what your job is, patients and other staff alike will invariably refer to you as “nurse” or “doctor”. Whilst doctors and consultants are prevalent in this career, it is difficult to convey to patients and staff, the differences between medic and scientist in both the hospital and these roles specifically.
This has highlighted to me, the need for a global identity and perhaps a way for we, as the people with that identity, to forge it for ourselves.
As the evolution moves ever forward, this blog may be named The Healthcare Scientist and I may be signing off with the same name.
We shall see.
I have this last academic year, completed my first full year of Cardiac Physiology.
My course consisted of four modules, each focusing on broad, yet still specific areas of science and scientific practice.
The modules were as follows;
Biomedical Skills.
– Medical physics, algebra, calculus, etc.
Anatomy and Physiology.
– Exactly what it sounds like; anatomical systems, terminology, dissection, prosection, and a hell of a lot of pop quizzes.
Physiology and Patient Care.
– The physics, biology and methodology behind various medical tests and how to use and perform them, then interpret the results, patient psychology and care, and the pathology of cardiac and respiratory disease, etc.
I refrained from creating this blog until the start of my second year due to the irrelevant content of the first year as a whole. Whilst the first three modules listed were required by the curriculum, they were far from ‘physiology-centric’ and the final module was little more than a (very good) detailed introduction. This will change, however, from here on out.
I must stress that this is not a slight on the course structure or its content so far, as nearly everything that myself and my colleagues have been taught has been engaging and informative, I simply felt that to document such a broad range of topics on a Cardiac Physiology blog would quickly become something akin to an unwanted university lifestyle diary. I can assure you, that aside from study tips, this shall not be the case.
The next steps of my journey are the ones that will be of greatest interest to fellow students, physiologists and hopefully to the relevant governing bodies.
In the forthcoming posts, I shall document my feelings on the course structure, content, struggles I have encountered and where the career path seems to be going.
I intend to post once a week without fail, but will update with more frequency as points of interest present themselves.
To those just starting their journey, I will post some relevant information regarding the Physiology module from last year, but mainly to assist with what’s to come.
If you know anyone who is currently journeying down this pathway, or is thinking of doing so, point them in this direction. I aim to network, exchange ideas, discuss common issues and everything in between.




 The P waves present in these altered leads are much more pronounced.
The P waves present in these altered leads are much more pronounced.