

TSP ECG #3
Male, 54 y/o

Comment on rate, rhythm, axis and anything abnormal you can find.
This quiz is a learning tool and is designed to promote discussion, so if you disagree with our analysis, sound off in the comments below; we’re learning, too!

TSP ECG #3
Male, 54 y/o
Comment on rate, rhythm, axis and anything abnormal you can find.
This quiz is a learning tool and is designed to promote discussion, so if you disagree with our analysis, sound off in the comments below; we’re learning, too!
The fact that this specialist degree exists primarily in universities is a relatively new event; before the shakeup by Modernising Scientific Careers, the majority of training was completed in-house with an element of distance learning thrown in to assist with the theory behind the practical concepts.
As physiological science makes the transition to a 100% university- led discipline, there remain students that are still learning the “old way”. Sarah is one of those people, and I had the pleasure of working with her this year during my rotations between respiratory medicine and cardiology. In order to get a bit of insight into exactly how the course differs between bases, she kindly agreed to be interviewed for TSP.

Hello Sarah! Could you outline the structure of your week, with regards to working in your department and studying the degree simultaneously?
I’m employed by the hospital, so have to work my set hours which are Monday – Friday 08.30-16.30. Although I’m studying, I am not employed as a student, rather, I am an Assistant Technical Officer, which basically means I help around the department doing admin, portering and some clinical work. I have certain responsibilities with regards to admin that I have to keep on top of regardless of what clinical work I need to be learning.
Monday is my main admin day, so I spend the entire day sorting through referrals, checking messages & booking appointments for certain procedures that only I book. I need to keep on top of this as some of the procedures have extremely long waiting lists, so if a patient cancels last minute I need to try my best to fill that slot. Once my admin is complete I normally help out my colleague in the office with some of her work load. If there is no porter to bring inpatients up & back for echocardiograms then it is part of my job to do this as well, which means I can’t get my necessary admin work completed.
Tuesday is the start of my clinical week, unless I have been portering the previous day. At the moment I am spending all day Tuesday in analysis, analysing 24 hour and 48 hour tapes. I am able to analyse a tape independently, but as I am still learning they all need to be checked after, just in case I’ve missed something or worded my report incorrectly.
Wednesday is a half day in the department for me as I have a collaborate session starting at 12.00 so I need to be set up in the library ready to start. After my collaborate session I catch up on any studying I need to do, such as looking over lectures that have been released for the following week, researching/ writing an assignment or revising for upcoming exams. On a Wednesday morning I will either be fitting ambulatory blood pressure monitors (supervised, as I am not confident to do them alone yet) or analysing.
Thursday mornings I am in Electrocardiography, either in the department or going down to the ward, and in the afternoon I analyse.
Friday mornings I do tape clinic which occupies the entire morning and keeps me very busy, especially if I have patients returning that have had symptoms of dizziness & I need to get the tapes checked before I can let them go. I spend Friday afternoons in analysis.
That is my current working week, but I will start going on the rota soon to sit in on exercise treadmill tests as well. Most mornings I get into work at around 07.30 so I can get some studying done before work and I try to do an hour or so in the evening as well. Most weekends I keep to myself, but if I have an assignment due or exams I will do a couple of hours each day.
That’s a hectic week. This might now be a silly question, but do you feel that this is this enough?
In terms of clinical exposure … yes! But it is very hard to keep up with the academic work load when there is very little time to fit things in. I commute for over 2 hours a day so this eats into my potential study time, but I try to keep a balance of work, study and actually having a life!
Do you feel that working in the same department as you study helps you to learn more and keep you motivated?
I feel that second year especially has helped me learn, but most of the academic work in our first year wasn’t particularly relevant to cardiology. I feel like I learnt more in the last 2 months from analysing tapes than I have in the whole 2 years that I’ve worked in the department. I definitely think it has helped to keep me motivated as I’m constantly surrounded by people that are doing the job I am training for, so I’ve got a clear goal at the end of it.
You’re one of the last sets of the distance intake. Do you think, if you had the choice, you’d still do the degree in the manner you currently are, or would you choose to be based at the university?
I’ve already done a previous degree so I’ve experienced the whole student life thing, so I’m not missing out by doing it this way. At the moment I am essentially being paid to learn, which is ideal. I wouldn’t be able to afford to do this degree if I was based at the university, as I’ve already had a student loan so I’m not entitled to another. I think I get a good amount of exposure in the clinical setting, but I just have to do some of the boring admin jobs to make up for it. At the end of my degree I will have a job and I know 100% that this is the career I want for myself. I wasn’t passionate about my previous degree subject so I lost interest and didn’t want to spend the rest of my life doing it, whereas I know from working in this department and from studying the way I am, that this is what I want to do. I don’t think I’d have that level of clarity if I was based more at the university than the hospital.
That’s fair. When we worked together during my placement, I was aware of the fact that you were much more comfortable in the clinic environment than I was (obviously), so what do you feel we at the university have by way of an advantage?
I definitely think that as I’m exposed to patients and the environment all day every day that I am more confident and comfortable than yourself, but I would say that full time students based at the university have a lot more academic knowledge. We have 1/2 hours a week of contact time with our lecturers so we need to go out and research ourselves, whereas it is clear that you guys have a lot more academic time although you miss out a lot with the lack of placement.
Thanks, Sarah!
As you can probably tell, despite the fact that Sarah and myself are in the same cohort, our academic years have a vastly different focus. As I (rightly) assumed just from working with her on the department, both routes present their pros and cons, and seeing as this is a vastly understaffed form of diagnostic science, it does, in my opinion, open the career up to a greater number of people now it will be university- led.
If you’ve got an opinion, or a question regarding anything you’ve read, sound off in the comments below.
Photo courtesy of Facebook

As part of our course we often perform ECG’s on one another to enhance and refine our practical ECG skills. During a practical recently I volunteered to be the patient so that my fellow students could practice their electrode placement skills; whilst being filmed and critiqued by others. The group universally agreed in the value of this experience, despite the fact it felt strange performing an ECG to an audience of your friends whilst being filmed in an artificial clinical environment. After everyone had practiced we printed of a recording of my ECG. Our lecturer, whom is a senior physiologist, explained that we would as a class analyse the ECG in our following lecture.
Upon the analysis of my ECG, my lecturer broke the news to me that I had left ventricular hypertrophy (LVH) with sinus bradycardia. Considering the previous lectures we’d had on LVH and its clinical significance I was pretty scared few a seconds or so. He then thankfully reassured me that in my case this was completely normal. My lecturer emphasised the importance of always combining your ECG analysis and findings within the context of your patient.
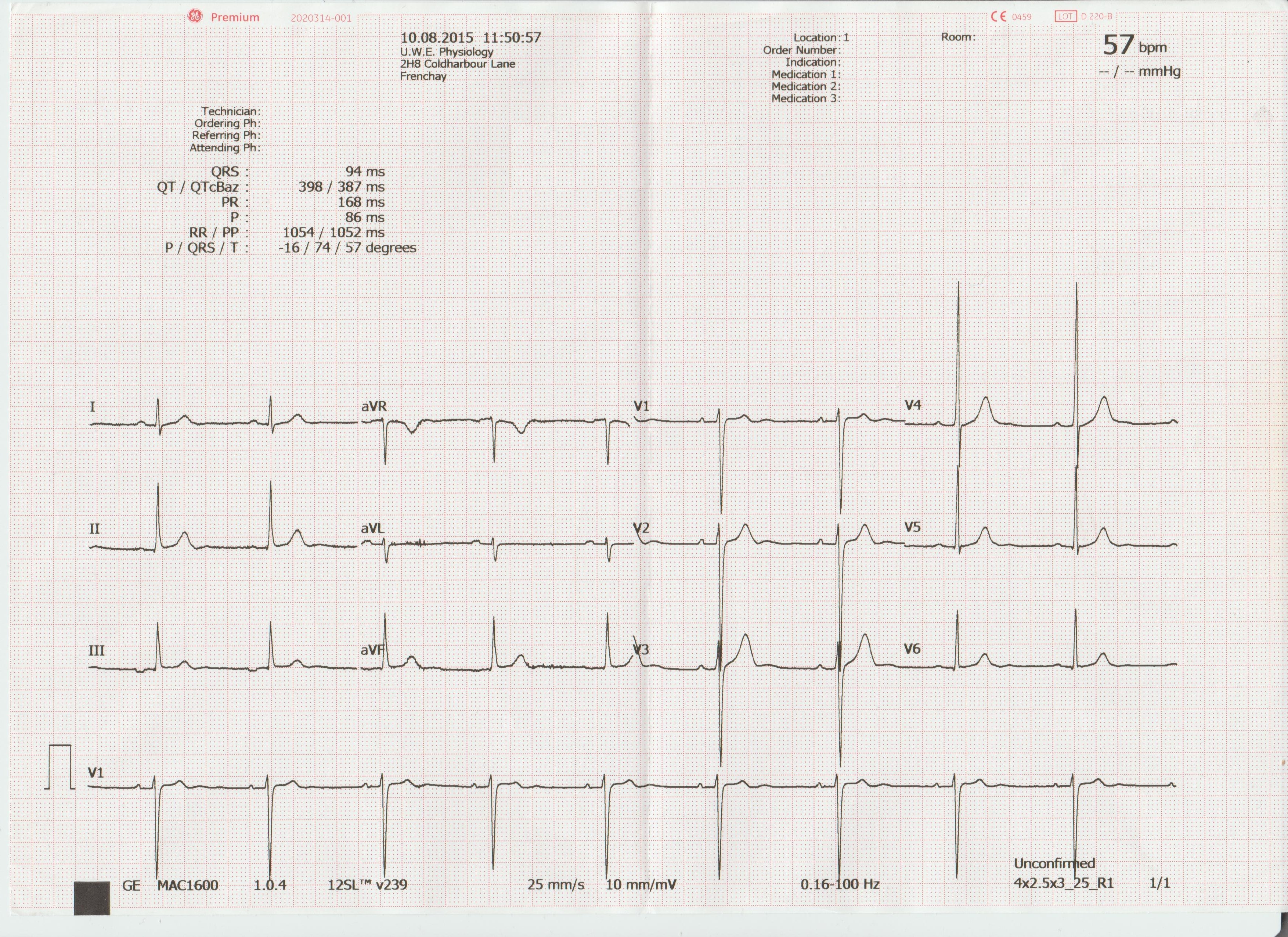
He explained my athletic physique (his words) and my age were enough to convince him that my development of LVH was not due to pathological reasons but that of heart remodeling as a result of prolonged physical conditioning. If presented with a 30 stone, 60 year old male, with LVH, or a 70 year old sinus bradycardic female ticking a long at 50 bpm and suffers occasional syncope; this would not fit as a normal finding in the context of these patients.
This practical highlighted the importance of always putting your ECG findings in the context of your patient and the normal ECG variants that may be encountered. The patients we see will be varied. They will be of different genders, ethnicities, ages, physical condition, possibly even pregnant. All these groups will produce significant normal variants in their ECG’s. These factors must always be taken into consideration when assessing the significance of your findings. Is your patient bradycardic and symptomatic suffering frequent dizzy spells or are they a young physically conditioned adult. We will be posting articles shortly on the normal variants expected in some of these patient demographics.
What is LVH
LVH is an increase in size and proportion of ventricular myocardium (in this case specifically the left ventricular myocardium). This can occur in any chamber of the heart but is most commonly found in the LV.
How is LVH diagnosed on an ECG
Most trained operators will spot signs of LVH relatively quickly on a ECG recording as it will be common that precordial ventricular tracings will overlap one another requiring a reduction in gain settings.
However, the Sokolow Lyon criteria is correct method of choice. This involves measuring the amplitude of the S wave in V1 and adding it to the R wave amplitude in V5 OR 6 (whichever bigger). If the sum amplitude is greater than 3.5mV LVH is suspected.
To calculate right ventricular hypertrophy (RVH): Amplitude of R wave in V1 + S wave V5 or 6. If the sum amplitude is greater than or equal to 1.1mV RVH is suspected.
However, an ECG alone cannot determine the extent of hypertrophy and its clinical consequence. An echo-cardiogram would be required to ascertain this.
Causes of LVH
LVH is a result of increased demand put on the LV to increase cardiac output. Over prolonged periods of time this increases cardiomyocyte size. As discussed earlier, this increased CO demand could be the result of exercise, and therefore sustained activity levels could lead to LVH. The upshot of this is that for every heart contraction the ventricles can force out a greater volume of blood for every beat (stroke vol) reducing the demand on the heart to supply cardiac output at rest. For this reason athletes with LVH will have a lower resting HR (sinus bradycardia).
However, there are also many pathological reasons for developing LVH, all of which result in pressure overload in the LV increasing its resting workload.
Some of the most common pathologies associated with LVH are as follows:
• Hypertension (most common cause)
• Aortic stenosis
• Aortic regurgitation
• Mitral regurgitation
• Coarctation of the aorta
• Hypertrophic cardiomyopathy
As LV hypertrophy develops, the myocardium can become so thickened that it begins to inhibit the filling of the LV reducing cardiac output leading to increased risk of mortality.
In my next article I will be looking further into some of the pathological causes of LVH and their clinical significance.
Ref:
http://lifeinthefastlane.com/ecg-library/basics/left-ventricular-hypertrophy/
I still haven’t.
Bear with me, though, as this is going somewhere, I swear.
After the last session, in which I provided the robot’s voice and controlled its HR and ECG, it dawned on me that as a result, everyone had the opportunity to be filmed performing the test and gain valuable group feedback, except me.
I wasn’t the only one to notice this, as it transpired.
During a subsequent lab session, wherein we practiced manual BP, honed bedside manner, discussed contraindications and compared different methods of BP measurement, it was revealed that the remainder of our ECG feedback period would be completed in the lab. We no longer had immediate access to the simulation mannequin, so thanks to a willing volunteer, another of my colleagues was able to complete the procedure and again receive feedback in a partitioned area of the lab.
Then it was my turn to step up to the plate.
I was the last to ‘go’, as it were. The difference between my assessment and the other’s lies in that everyone else enjoyed an element of seclusion: the curtains around the bed-space being pulled in the first session and the high walls that separated one section of the lab from the other, in the second. The rest of the group stayed outside of these boundaries in everyone else’s case. Not for me, though. I stood away from the couch, preparing to make my entrance to the imaginary treatment room I could see in front of me and just before I could open the invisible door, the consultant physiologist taking the session said “Wait, I’m just going to call everyone else in, if that’s ok?”
“…If that’s ok”, as if I had a choice.
Everyone else filed in. They kept filing in for what felt like an age. My lecturer, the rest of my class and the head of physiology. Then, they all looked at me, waiting.
I’m not sure how I’d have fared if I’d known this was going to be the format for my peer assessment, but I feel no shame in admitting that I don’t remember ever being as scared as I was before I started moving. I didn’t know how to begin, so I just went for it. I walked into the ‘room’ (after, somewhat embarrassingly, opening the invisible door) and performed the test as I would out on placement.
I asked all the required questions and added one or two patient identifiers to account for the fact that I didn’t call my patient from any waiting room and gained a consented, accurate trace.
Not only did I do it all with the eyes of more than a couple of people scrutinising my every move, I did it with a piece of equipment I have never used before and the most tentacle-like cable configuration I’ve ever seen in my life- if you’ve tried to untangle the wires behind your television when you’re moving house, you’ll know what I mean but, trust me, this was worse. In addition, I managed to ignore a completely new experience: the fact that I was so scared that the back of my neck was sweating..!
Fear is natural. It’s normal to be scared of doing something that’s relatively new to you, especially when you know you’ll be watched and judged doing it. Whatever ‘it’ is, it wouldn’t feel like a real achievement if we didn’t feel fear beforehand. I’m glad it was sprung on me, if I’m honest. My final assessments and various practical examinations for the rest of my career will follow this format so it’s good to have a grasp on some of the emotions I’ll be feeling before them. If you’re just beginning the PTP programme, you’ve got things like this to look forward to, so just try to enjoy it. Realise that the fear of these things is normal and, most importantly, the sooner you take a deep breath and swallow the lump in your throat, the sooner they’ll be over!
Thanks!
Hello again!
It seems that as soon as I mentioned just how quickly this profession is evolving, something has been raised that enables me to give you an idea of how much.
This blog is called The Student Physiologist. The career’s professionals are known as physiologists or physiological scientists, ergo, myself and my peers are subsequently coined physiology students.
This, however, will soon be a thing of the past, as by the time I qualify, these terms will no longer exist. In their place will be Healthcare Scientist.
It’s difficult to find any sort of identity in such a changing professional environment and this difficulty is bolstered when a physiological scientist tries to explain their role within the NHS. We are among the most patient-facing scientists in the clinical setting, yet we are arguably the least “seen”, in that no matter the description of who you are and what your job is, patients and other staff alike will invariably refer to you as “nurse” or “doctor”. Whilst doctors and consultants are prevalent in this career, it is difficult to convey to patients and staff, the differences between medic and scientist in both the hospital and these roles specifically.
This has highlighted to me, the need for a global identity and perhaps a way for we, as the people with that identity, to forge it for ourselves.
As the evolution moves ever forward, this blog may be named The Healthcare Scientist and I may be signing off with the same name.
We shall see.
Thank you.
Hello.
I have this last academic year, completed my first full year of Cardiac Physiology.
My course consisted of four modules, each focusing on broad, yet still specific areas of science and scientific practice.
The modules were as follows;
Biomedical Skills.
– Medical physics, algebra, calculus, etc.
Anatomy and Physiology.
– Exactly what it sounds like; anatomical systems, terminology, dissection, prosection, and a hell of a lot of pop quizzes.
Cellular biochemistry and Genetics.
– Microscopy, mrganic chemistry, pharmacology and, shockingly… Genetics.
Physiology and Patient Care.
– The physics, biology and methodology behind various medical tests and how to use and perform them, then interpret the results, patient psychology and care, and the pathology of cardiac and respiratory disease, etc.
I refrained from creating this blog until the start of my second year due to the irrelevant content of the first year as a whole. Whilst the first three modules listed were required by the curriculum, they were far from ‘physiology-centric’ and the final module was little more than a (very good) detailed introduction. This will change, however, from here on out.
I must stress that this is not a slight on the course structure or its content so far, as nearly everything that myself and my colleagues have been taught has been engaging and informative, I simply felt that to document such a broad range of topics on a Cardiac Physiology blog would quickly become something akin to an unwanted university lifestyle diary. I can assure you, that aside from study tips, this shall not be the case.
The next steps of my journey are the ones that will be of greatest interest to fellow students, physiologists and hopefully to the relevant governing bodies.
In the forthcoming posts, I shall document my feelings on the course structure, content, struggles I have encountered and where the career path seems to be going.
I intend to post once a week without fail, but will update with more frequency as points of interest present themselves.
To those just starting their journey, I will post some relevant information regarding the Physiology module from last year, but mainly to assist with what’s to come.
If you know anyone who is currently journeying down this pathway, or is thinking of doing so, point them in this direction. I aim to network, exchange ideas, discuss common issues and everything in between.
Thank you.


