It’s my third week of my penultimate year’s clinical placement, and I‘ve analysed nine tapes, unassisted. This whole piece of reflection took a great deal less time for me to write, than completing an analysis of a Holter recording does, but it’s only week three, so I didn’t expect much more. In fairness, I didn’t expect to have become this comfortable with the analysis software quite so quickly, but this placement has already been filled with pleasant surprises, so I’m just going with it at the moment.
I will add that the feedback gained from these completed reports has been extremely positive, which is a bonus. The returned work has been annotated, informing that my rhythm recognition and ability to use my knowledge to correct the computer software is excellent, as is my report structure and clarity of information. Given areas for improvement highlight my initial propensity for forgetting to include basic rhythm strips (saying it’s sinus is fine, but it has to be proved), and learning the nuances in the software itself.
This, I have found to be the most difficult thing in the entire analysis process; Pathfinder is an incredibly user-friendly piece of kit, for the most part, but there are certain aspects of its functionality that don’t make a jot of sense to the beginner; certain screens don’t allow for 3 lead strip printing (even if you select it), selecting a beat to reclassify doesn’t always give you all of the different classification options, rather, it presents a select few, and (in my case, at least) 90% of the time they aren’t what you want to reclassify as, and perhaps most bafflingly, it reclassifies each event category as you analyse; on a few occasions now, I’ve reached the end of a tape, only to find another 30 un-viewed events have appeared in previously completed categories. Being aware of these things is vital, but don’t take too long to get to grips with, however.
Receiving feedback on completed reports is nerve-wracking, especially when they’re being marked right next to you. I have noticed, however, that everyone (literally EVERYONE) has a preferred way of writing a report, and classifying certain beats. Below, I have provided an illustration of an event I encountered in a 48hr recording: Pathfinder had classified this as a ventricular triplet, but I noticed there was a pause between the second and third beats indicating a couplet with a compensatory pause, followed by a further single ventricular ectopic. I had never encountered this before, so erring on the side of caution I asked a colleague for advice. I was informed to go with the software in this instance, as it most likely was a triplet. In essence, I was told that as long as I highlighted it in my report, then it would be visible.
After taking this advice, I submitted my complete report, only to be informed that my initial assessment was correct; it was indeed a couplet followed by a pause and another PVC, but that people would have different opinions on such a subjective event, so it wasn’t a big deal.
Whilst writing this same report, I used the cardiac event frequency guidelines suggested by my trust;
Rare = <15 per hour
Occasional = 15 – 30 per hour
Frequent = >30 per hour
For analysis of a 24hr recording, for example, 263 single ventricular ectopic events across the whole tape would give just under 11 events per hour, so these would be reported thusly;
Rare PVCs seen singly
If, however, the majority of these beats were recorded between 5 and 7 pm (i.e. more than 30 per hour for this given period), the above report would need to be altered.
I have employed this structure:
Rare PVCs seen singly (frequent between 17:00hrs – 19:00hrs)
This style documentation has been approved by some, but not by all. The marking that has been returned to me thus far has been as subjective as the reading of a difficult 12-lead ECG, so I’m not entirely sure what to go with as yet. Some have instructed me to use full sentences in this instance, others say that I’ve included the perfect amount, and ALL have said that the subjective nature of this marking is inescapable, so I’ll have to get used to it, as if I change my report style now, I’ll get the same divided comments, only in reverse.
Wording aside, I’m both pleased and excited with my progress already, so hopefully I can overcome these few hiccups in the weeks to come.
I had the rather marvellous opportunity today; spending a day in cardiac theatres and, under the guidance and tutelage of two cardiac surgeons and an anaesthetist, learning the processes and methodologies behind CABG and MV repair.
I arrived at the Bristol Royal Infirmary surgical centre at 7:45am and was quickly changed into some scrubs and inducted into the OR’s team: three surgeons, two anaesthetists, one perfusionist and a selection of nurses both scrub, and regular. It was clear to me that each of these individuals knew one another well, just by the way they talked to each other; everyone seemed at ease with the rest of their colleagues. It turns out, I was right. Many of them knew each other from other hospitals, university or simply having been mentored by each other during training. This camaraderie bled into the surgery, as each team member knew not only their role, but that of the others, also, so equipment was passed over or set up without being requested, making for a seamless procedure.
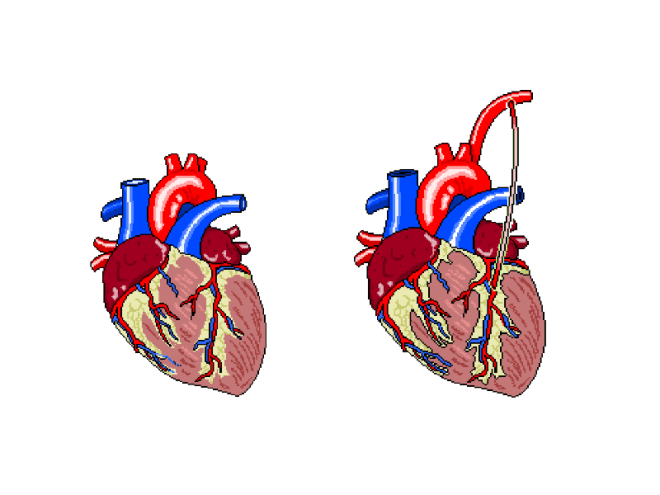
The patient was, until the last year or so, a very fit and active 79y/o, who had suffered from AF for at least 10 years, and had developed a stenosed left anterior descending coronary artery as a result. In addition, echo had shown a severe mitral regurgitation due to valvular prolapse. The procedure would attempt to bypass the LAD using the left internal mammary artery (LIMA), as shown below.
Figure 1: The left internal mammary artery (shown in situ on the right) is relocated from the chest wall to bypass the stenosed section of the LAD.
The plan was to perform the bypass graft, and then set about repairing the damaged mitral valve.
After the patient’s ID and contraindicators had been checked, the anaethetists set about carefully monitoring their respiratory and cardiovascular function as the GA took effect. The ECG, arterial and venous pressure traces were available on lots of screens around the rooms, as whilst they must be monitored all of the time, it becomes particularly important to keep an eye on the given values as the heart is both stopped and re-started.
Interestingly, I noticed a pattern in conversation with each patient throughout the day, as the anaesthetic was administered. The patient was asked to think of their favourite place and the team then asked where that place was. Each time, this was met with silence, but just to make sure, the patient was always asked if they were warm enough. When no answer was forthcoming, they were wheeled into the theatre room proper.
Not everyone on the team was scrubbed up and sterilised, as obviously some would not be required to touch the patient, and others would be required to fetch replacement equipment should it be needed. This created a “sterile field” around the operating table, so only sterile members of staff were permitted within it.
After 1 hour and a whole heap of sterile gowns and drapes were applied over the patient, with only a small window showing the surgical site, the operation began.
Step 1 required access to the thoracic cavity. In case of blood splatter, masks fitted with facial protection were supplied to myself and the other team members who would be in the direct vicinity of the patient when the chest was opened.
An incision was made as illustrated below. This is known as a median sternotomy, and extends from the sternal notch to the xyphoid process. In order to progress past the sternum, an oscillating saw is used to cut throught it. There is a surprising amount of finesse involved in this stage, despite how much pressure is required and as a result, how brutal it appears.
The incision is deepened and cauterised until it travels through the pericardium, so as to allow access to the heart and, after the bleeding vessels around the wound are cauterised, a finochietto retractor is used to hold the sternum open. During this time, the LIMA is found and carefully removed from the chest wall. It is then held in an accessible place with forceps, to be used later.
Lung and cardiac function is transfered to a cardiopulmonary bypass machine, which allows both the heart and lungs to be stopped/emptied, allowing even greater access to the heart due to the lack of lung obstruction, and intricate work to be perfomed whilst the heart is not beating.
The cardiopulmonary bypass apparatus purifies the blood that passes through it from the patient via cannulas placed in the heart and pumps it back, thereby doing the work of the heart and lungs. The heart is fed nutrients at the same time, so as to keep it healthy for the extended period of inactivity. This method of on-pump surgery is known to be incredibly safe- between 1 and 2% of high risk patients will suffer adverse effects as a result of the treatment, and surgical teams are well versed in assessing this via risk factors.
Once the LAD has been correctly identified, an incision is made, creating an opening that roughly matches the size of the end of the LIMA, and the two are stitched together using sutures made of polypropylene,which are no thicker than a human hair, yet can withstand the pressure that would be required to rupture a healthy vessel. To test the suture site, blood is passed through the vessel, and in the event of any gaps in the connection, this blood will be seen outside of the join, which can then be further secured as necessary.
The process, whilst quick to document, was a long one, as each step of the technique was scrutinised carefully before considered complete. In addition, each stitch required at least two people directly, to exact it; one to add the suture, and the rest to support the structures surrounding it.
The second stage of this case was the mitral valve repair, which was in itself a multi-stepped procedure. It is possible to repair a damaged mitral valve using less invasive, keyhole methods, but due to the need for a bypass graft, this wasn’t an option this time.
After gaining access to the valve itself, via an incision in the left atrium, the condition of the valve leaflets is assessed. This particular patient’s posterior leaflet had a prolapsing middle scallop, which meant that the below procedure was necessary to repair it.
The process off attaching the ring was a long one, involving a lot of organisation and intricate knotting. The sutures are applied to both the ring and the valve, the latter is then gently pushed down the threads and into place. These suture strings are then tied off and cut.
Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.
When performing the annuloplasty removed the surplus anterior leaflet, it took with it a tendineae chordeae, so in order to stabilise it further, an artificial heart string (made of Gore-Tex) was attached to the leaflet and papillary muscle.
A final transesophageal echo was performed, to assess the level of air still present in the heart, and to then assess the function of the repaired mitral valve, and after all of this was successfully accomplished, the long task to gently remove all of the cannulas that were used to bypass the cardiopulmonary system were begun to be removed. Each chamber was sutured in sequence, and the corresponding section of the perfusion apparatus turned off. All of this time, the anaesthetist monitored the patient’s drug infusions and every member of the team monitored pressure and ECG traces. This was still going on whilst the SpR set about cauterising vessels and wiring the sternum before pulling it back together. None of this section of the procedure involved any real finesse; pulling the wires taut so as to close the chest cavity is a test of strength. Each pull caused the patient to move for the first time since coming into the theatre, so I guess that was why it was the only section of the surgery that almost made me wince (something the theatre lead noticed and laughed about). Once it was done, the multiple layers of sutures were applied to seal the surface wound and the patient was taken to recovery.
In all honesty, the most difficult part for me, was in standing for so long. This was echoed by the surgeons, who said that they always felt backed up by their colleagues, so they felt confident that the procedure itself would go well, but standing, often in an unnatural position for so six hours at a time played havoc with their backs and legs. The anaesthetists, being required fully at the beginning and the end of the surgery, spent a great deal of time sat waiting, save for occasionally changing an infusion as and when required. The people working solidly were the surgeons and the scrub nurse, but even the surgeons swapped roles, observed one another without participating, and even took breaks periodically. None of this diminishes any one role, however; each member of the team was required, be it constantly or otherwise, and when one was needed, it took a single word for everyone in the room to know what was required, and by whom. Despite the procedure itself being amazing, it was the mechanical and seamless nature of the professionals in the room that was the most astounding part of the day.
Exams are over, coursework is in, and I’ve FINALLY got some time to devote to TSP, so I’ll endeavour to post updates with the same level of regularity as I did a few moths ago. It’s been a while since I added anything other than study pages, so it’s proving difficult to get back into the swing of reflective writing. I shall try to be clear, however.
The first week of my 15 week placement has been an interesting and challenging one. I’ve been in pacing clinics (the third of which allowed me to have some hands-on experience), tape clinics and have analysed my first full 24 hour ECG recording, so the amount of information I’ve absorbed has been of a high volume in a short space of time.
I’m not going to comment on tape analysis or clinics just yet, as I’m yet to have my completed work assessed, so I’ll wait until I’ve gained some feedback on my current performance. Pacing, however, is extracurricular, so I’ll glady share my experience.
Pacing checks were very fun; during eight or so hours of lingering/observation, I was gradually allowed to do a bit more with regards to clinical practice; analysing lead outputs and EGM readings, setting up programming equipment and learning my way around each box-specific bit of software, etc.
The majority of patients that came into the clinic were annual follow-ups, and six week post-insertion assessments, wherein the overestimated pacing parameters are altered so as to preserve battery life, and due to their nature, each was simply a case of checking each value and adjusting accordingly, meaning each 15 or 20 minute consult went off without a hitch, and I got a feel for the regular procedure and could have some of the physics explained to me. It also allowed my tutors to ask me questions and test me a bit.
The third and final clinic, however, allowed me to assume the role of primary (under strict supervision, of course) and perform threshold tests on my patient. It’s amazing how quickly it’s possible to forget everything you’ve spent the last few days learning, when it comes to actually doing it; the sudden pressure of being thrown into practical learning caused my mind to go completely blank, but with a bit of time, I settled into the role and things started to make sense as I was doing them. There’s a really overwhelming feeling of resposibility when you’re charged with manually increasing or decreasing your patient’s heart rate during threshold tests, and in addition, spotting the loss of atrial capture is, in most cases, far more difficult that that of ventricular capture. It was an exillerating experience, though, and I really felt like I had accomlished something at the end of the clinic. In three days I felt like I could quantify my progression, so the first week has left me feeling excited for the rest of the placement block.
Until this week, I’d never considered pacing as a future specialism – I was focussed on echo – but getting some real exposure has shown me how much I could enjoy a future in the discipline. I can’t wait to do more.
I’ll write more about my own research into pacing as I do it, so keep an eye out for that.
Synap is an upcoming revision tool that is driven by students. The platform enables students to create their own multiple choice questions and upload them, then download those created by others. It’s possible to “follow” other users, as you would someone on Twitter or, incidentally, this site (you can do that in the sidebar of this page…), and take any quiz that they have created. Image upload and basic editing is supported, so quizzes for physiology, such as ECG arrhythmia or echocardiography quizzes are more than possible, and are one of the reasons I decided to get involved with the whole thing. In addition, the app tracks your progress and structures your revision for you, based on your course and modules.
I’ve spent the last week or so beta testing the Synap web platform or, more specifically, I’ve been taking tests and creating basic ECG quizzes to help bug test and check functionality.
The platform, as I’ve mentioned, is currently in closed beta and only present on the web, so without having an app and a larger number of users I cannot comment on it fully, but as it stands, the processes involved in creating a profile and quiz are incredibly simple; adding and annotating images is a cinch, and a complete question only requires the user to add a correct answer and a few wrong ones. Whilst I encountered a few bugs initially, the feedback I provided was swiftly taken on board and the problems were remedied overnight. Taking quizzes is incredibly simple, and all you need to do is click “take quiz” (shockingly), then select your answers and have them marked. You can take these as many times as you like, too, and if the creator has provided any, feedback will be available for each individual question.
My only concern is the reliance on the quiz-maker supplying the correct information. I’ve taken a quiz wherein the correct answer was the only one that was possible to be correct (think “What has tusks and a trunk? 1) Elephant 2)Belephant 3)Your hamster”) yet I was still told my answer was wrong. This is a closed beta, though and that’s what these processes are for. I know it hasn’t escaped the attention of the developers, so we shall see how it is dealt with.
To break all of this down and show you what I know for sure so far, have a look at this (incomplete) features list:
MCQs:
Image/annotation upload
Correct answer & up to 5 incorrect
Optional feedback for test-taker
Optional link to external learning resource
Test result calculation
Obtainable achievements
Personalised revision quizzes sent to you
Community links based on:
Course/Discipline
Cohort
Institution
I’ll add to this list the more familiar I become with the platform.
Omair and James, its creators, and the rest of the Synap team hope that this app will enable students nationwide to help each other and revise together, and it’s a pleasure for me to be involved, even if it’s only in a small way, currently. I’ll continue to post updates as things progress.
As with part one, the procedure itself will not be detailed, as it is not under discussion, currently. My experience as a patient will be the focus, so I will relate my experience back to those who you will be performing these tests on throughout your careers.
After part I, my legs- nay- my whole body ached, so I was looking forward to my echocardiography patient experience, as it would not only give me an idea as to my heart’s structural health, but also give me a bit of lie down…
Unlike those patients who have never undergone an echo procedure, I knew what to expect, as I had observed more than a few and have had a go at one before, but I was still apprehensive, given the required level of undress and the fact that I had never had one before. I had an idea that my heart was in fairly good condition, but you never know for sure until you have results so as you can imagine, for a patient with a suspected pathology the time spent waiting for the test is a nerve-wracking experience.
Hearing people talk about what they can see on images of your heart that, due to the angle you are often required to lie and that of the monitor, you can’t see, isn’t wholly pleasant, so it was easy for me to further empathise with patients having the procedure themselves. In addition to this, the feeling of exposure is made worse by the positions one is required to remain in; my hips, shoulders and legs were uncomfortable to the point that they hurt after 20 or so minutes. Guidelines recommend that an echo procedure takes 45 minutes, and whilst a patient is supine for some of it, an elderly patient, or one with previous limb surgeries will likely find the scan more painful than I did, especially when required to roll onto their side.
There is an odd feeling of one’s personal space being invaded, as the practitioner has to reach across the patient’s trunk in order to reach the designated areas for scanning, which further adds to the discomfort.
These things combined, meant that my longed-for lie down, was not as relaxing as it could have been. Throw the anxiety that comes with a) being in a clinical setting, and b) awaiting a verdict on your heart health/ a pathology, and I can only imagine how much more uncomfortable an experience it is for patients.
My echo and stress test experiences have shown me that, even when procedures are at opposite ends of the patient participation scale*, patients have to endure a great deal of discomfort. Even though echo is physically non-invasive, it comes with a heap of emotional distress, so when you’re out on placement, just think about what your patients are going through.
If you’re having a bad day, remember that, even if their visit is routine, due to simply having to be there, your patient’s is probably worse.
(or “what I learned when the tests I have done to others, were done to me”)
The tests presented in this post are intentionally not explained thoroughly here. I have focussed, currently, on patient experience. If you wish to learn more about the things presented here, and the interpretation of the possible results, wait for them to be explained in your lectures, or, perform a quick Google search.
Before the new semester began proper, I was asked to assist with some physiology practicals on my campus. I agreed because I felt (much in the same way a chef will sample his/her food before selling it to the masses) that it would be good for my overall learning to experience the same anxieties and physical exertions -if applicable- that a patient may endure when they undergo physiological testing. When one repeatedly performs tests day in, day out, it’s easy to forget that the patient likely does not have anywhere near the same levels of familiarity with the procedure and proficiency with them as that of you, the practitioner, so to gain an insight into the emotional and physical aspects from the other side would, I felt, be good practice.
Day one was one of a cardio nature, in that I performed lots of exercise tests at a physiologist’s disposal. (Some of these tests are reserved for respiratory physiologists, but if you’re studying and are not yet at the point of choosing which PTP pathway to follow, you’ll experience these, too).
I discovered upon entry, that I would be performing the following:
YMCA step test
Bleep test
Treadmill test: ramp protocol (similar to the Bruce Protocol)
The wait to enter the lab was, (obviously not the same in terms of anxiety levels, but regardless) akin to a patient’s wait to enter a clinic testing room; knowing that I was going to have to perform tests, but not knowing exactly what they were was rather nerve-jangling (especially considering my then-unknown weight gain after the obligatory food-filled, sedentary lifestyle commonly experienced over the festive break).
The real difficulties stemmed from trying to comprehend the techniques required for each test. Explaining, or writing about them is one thing, but actually doing them is another thing entirely.
The YMCA step test itself wasn’t particularly challenging, given that it only involved 3 minutes of steady box steps. The difficulty came in not influencing heart rate on recovery. Knowing that my HR was being documented every minute meant I kept looking at the oximeter, and as has been documented (a quick google search will give you confirmation of this), it is relatively easy to change your HR on command.
For a patient, this last point may not be of particular issue, given that they might not be particularly aware of the potential influence they can have on their HR, but I can easily see how repeatedly stepping onto and off of a box could be difficult task for a patient of advanced age.
Bonus Clinical Perspective: In this test the Heart Rate Recovery and VO2 max doesn’t appear to be particularly accurate, when using normal values, especially when compared with the VO2 max displayed through the other tests, either. The values are based on age, as oppose to individual physiological characteristics, so assume a physical ideal that doesn’t necessarily transcend to real life.
The bleep test wasn’t like ones I have previously attempted in the gym, or what have you; rather, it was more about timing, ensuring there were no stops. This involved slowing down so as to reach the end of the designated track in time with the beep, then speeding up to repeat, meaning that pacing yourself was a must. The resulting strain on my legs caused them to become incredibly painful, incredibly quickly..! (I’m aware that bleep test procedure differs between fitness centres, so forgive my whinging if you use this format regularly).
Encouraging a patient to exhaust themselves doing this test would take a great deal of commitment from both parties; I’m not particularly unfit, but I had nothing tangible to aim for, with regards to an end point, so with no time to “beat”, I didn’t have anything to work towards and as a result, I gave up after 10 or so minutes, despite the fact I could have carried on for a while longer. For the average patient that would frequent clinics to perform this test, achieving maximal exertion may not be something that can be coaxed out of them, especially if they had already endured other tests in the same day.
Already I was beginning to understand the plight of the patient, when it comes to tests that require their full participation, and I still had the hardest one to come… I was not looking forward to the post-lunchbreak activities.
It turns out, the Ramp Protocol test was actually the most enjoyable of the day. Perhaps this was simply because I was growing used to being fatigued/dehydrated, or perhaps it was the setup of the test itself, but I could have happily continued running on the treadmill for a great deal longer than I did, time allowing.
The ramp protocol treadmill test involves the face mask setup presented in the pictures, and a steady speed and incline increase on the treadmill for as long as it takes for the patient to reach their VO2 max, but it is up to the patient when they stop. Unlike the bleep test, which involved travelling at an uncomfortably slow rate at times, the ramp protocol was a fairly rapid journey to a pace similar to that of a distance runner. It was far from comfortable, so would still require a great deal of coaxing and encouragement in order to get the patient to work hard to complete the test, but it was certainly more comfortable than the test that had preceded it.
The whole day not only reminded me of tests and theory that I had almost forgotten, but it really helped me to understand what a patient has to go through when they visit a hospital. The feelings and tests that I personally experienced were, on the whole, not pleasant, but I wanted to be there. For a patient, this will most likely not be the case. When your clinic list is seemingly never-ending and you don’t have time for restarts, it’s easy for the fact that patients don’t know the requirements and procedures as well as you might, to slip your mind, but thanks to this experience, it’s something that I’ll never forget, and I feel it solidifies a vital skill that students require to be able to operate efficiently and fairly: empathy.
Tomorrow brings a different kind of discomfort, in that I will be having my first echocardiogram. I’ll add that experience to part II
The ramp protocol will also get the full write up treatment, as it was by far the most complex and in addition, I have a detailed set of results.
This quiz is a learning tool and is designed to promote discussion, so if you disagree with our analysis, sound off in the comments below; we’re learning, too!
During the festive season, its easy to indulge in excess; too many sprouts, an increase in afternoon napping, festive drinks… You know the score. It isn’t all smiles and sunshine, though, as we shall see.
One particular result of all the festive excess relevant to cardiac professionals, has been reported across the globe, but particularly in Entirely Fictitious Primary Care Centres (EFPCCs); Bacardi Branch Blocks, or BacBBs
BacBBs are thought to affect the heart as a whole, but it can be seen that they have a particularly odd effect on the ventricles, and cause an odd, never-seen-in-real-life depolarisation wave on the ECG, that actually defies physics and medical science by going back in time!
Symptom sheets compared with the compiled ambulatory data have shown unanimously that BacBBs are present sporadically within sinus rhythms, but coincide with that one-drink-too-many during a family game of Monopoly (Mr Moneybags isn’t thought to be an underlying cause, so the activity isn’t seen as a risk factor).
Atrial activity stops altogether, presumably because the SA node just forgets what it’s doing, as it’s seen enough crepe paper hats and screwdriver sets fly from crackers to last it a lifetime.
After an episode of BacBB, sinus rhythm resumes, and the patient will return to whatever their festive-norm may be until the next instance.
This phenomenon seems to disappear entirely during the first couple of weeks of January, when normal working hours begin again, hence, I feel that it is triggered by the holidays themselves.
None of this is being researched, or is even disputed, because it is both totally false, and invented entirely by me.
Bacardi Branch Block
Common holiday rhythm abnormality only found during the festive season, and even then, only in fictitious settings
HR between 80-120bpm
Depends entirely on board game leader-board position
No P waves
Abnormal ventricular action
Resembles upturned cocktail glass
Is thought to only contribute to familial tolerance levels during prolonged exposure to each other
HAPPY HOLIDAYS FROM EVERYONE AT THE STUDENT PHYSIOLOGIST!!
This quiz is a learning tool and is designed to promote discussion, so if you disagree with our analysis, sound off in the comments below; we’re learning, too!
I never considered just how difficult trace analysis could be. Don’t get me wrong; I knew it would be hard, I just didn’t fully appreciate quite how hard.
During lectures on specific arrhythmias, when ECGs are displayed, they generally contain the abnormalities that make up the subject matter so it doesn’t take long to come to the correct answer, but looking at a trace without any history or prompting as to the condition, is still overwhelming to me. So overwhelming, in fact, that I often feel like I’m falling short of the mark with regards to my learning as a whole. The TSP ECG section is as much for my benefit as it is for you guys, in that I’ve found analysing the ones selected for posting incredibly difficult.
No matter what answer I come to, there’s always the lingering worry that I’ve missed something.
How much is too much, with regards to analysing?
What’s a result of over-analyzing, and what’s accurate?
Textbook traces, whether clinical, or stylised, have been selected as the best possible example of the rhythms under scrutiny, so it stands to reason that they won’t exactly mimic those that will be encounered in the field. In my limited experience, clinical traces contain a great deal of variation and have thus far, rarely resembled anything you’d find in a book.
They have been difficult, yes, but they have also been possible. This will all become easier, with practice (I assume/hope), so I hope you all find the analysis quiz good practice, as it’s certainly proving to be that for me.


 Pathfinder had classified this as a ventricular triplet, but I noticed there was a pause between the second and third beats indicating a couplet with a compensatory pause, followed by a further single ventricular ectopic. I had never encountered this before, so erring on the side of caution I asked a colleague for advice. I was informed to go with the software in this instance, as it most likely was a triplet. In essence, I was told that as long as I highlighted it in my report, then it would be visible.
Pathfinder had classified this as a ventricular triplet, but I noticed there was a pause between the second and third beats indicating a couplet with a compensatory pause, followed by a further single ventricular ectopic. I had never encountered this before, so erring on the side of caution I asked a colleague for advice. I was informed to go with the software in this instance, as it most likely was a triplet. In essence, I was told that as long as I highlighted it in my report, then it would be visible.






 Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.
Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.