A cardiology fellowship will give you the opportunity to be fully prepared for the field and can go as long as four years. It will help you to hone your clinical skills and have cutting edge skills in surgery. A mix of research, public lectures, clinical experience, and classroom-based learning all combined enable one to be very well versed in the field at hand. Fellowships in Cardiology range from Cardiac Surgery Training, Cardiac Critical Care and Paediatric Cardiology, Vascular and Interventional Radiology, and Vascular Surgery and Endovascular Therapy Fellowships.
Several institutions offer what are considered the best Cardiology Fellowship Programs. To choose and get accepted into the best cardiology fellowships programs successfully, requires much more than an exceptional personal statement; applying to a residency, especially a cardiology one, is challenging and requires a lot of work. The existing places for such mentorships are extremely limited and contested, so you have an obligation to be unique and to stand out in order to be accepted.
Your cardiology fellowship personal statement is an opportunity whereby you can say why you feel you are the most deserving of being enrolled in the program. Elevating yourself above the bar will determine whether you are accepted or rejected. Here you will find the help to writing a personal statement for fellowship in cardiology, as well as some dos and don’ts.
Fellowship goes above and beyond a good resume. A good resume can only go a long way. You can be the most qualified and have the best CV, but this will not guarantee you a spot in the fellowship program. As a candidate, do research on your options, enhance your exposure on volunteer work, conduct clinical research projects, and get publications. Ensure that you have filled the gaps in your resume and took the time to address all of them practically. Most candidates limit their options depending on where the hospitals are situated. This approach is detrimental, however, and prevents them from having a varied list and therefore options pertaining to the top-notch institutions. As a candidate, you can polish up your resume with a clearly defined and well put together personal statement.
The AMA or the American College of Physicians. Most candidates are not part of any corporate entity that advocates for their medical practice. With the continuous cutting of funds in the national budget, it is getting harder and harder to provide any services. This, in turn, has reduced the number of applicants able to be accepted and therefore numerous candidates find themselves being turned down. Joining the AMA will help you get a fair trial and increase your chances of getting approved.
Application to highly competent residency. Programs in radiology, dermatology and cardiology are highly competitive, and the stakes are high. Some of these students’ performances in their former medical school are usually not up to standard and sometimes place few schools on their ranking list.
Expansion of classification list. Students tend to limit their options and apply to a few residency programs. However, it is encouraged that a student lists down at least five hospitals to increase their chances of getting accepted. These choices can either be within their chosen specialty or even selecting a different specialty.
Transitional slot. A student can contact their medical school and ask for an interim slot or see a research fellowship. With this, the candidate will be able to become more competitive in the field and increase their chances of approval. An additional degree is also a supplement to a candidate’s resume and consideration.
Ill-preparedness. Two or more years of postdoctoral training whereby there is formal coursework in the fundamental sciences pertinent to the investigator’s area of expertise; this increased chances of attaining a fellowship.
Medical residency interview. It’s like a pass mark for all residents. Most programs won’t absorb candidates they have not interviewed. It is crucial that you take this interview seriously as it will not only determine if you will get accepted but also where you will get accepted.
Robin Dale is a junior doctor and her passion is guest post writing. She is fond of writing useful posts for students to make their learning lives easier and more effective. Her own life credo is “Keep calm, study hard, and become a doctor”.
EDIT: The Android version of TSP Mobile: ECG is available for download, but due to the way in which Google Play operates, I have been unable to offer it for free. The iOS version, when available, will be gratis for the promised 14 days however. Still no word from Apple when that will be, but I have been assured that it is being vetted as I type this, so fingers crossed!
Original article follows:
Well, that TSP mobile app I promised…
I’ve been saying I’d do it for months and, despite remaining fairly quiet with information about starting, I actually have been working on it. So much so, in fact, that the bulk of the development is finished! It’s in final stages of testing, after which it will be available on the Google Play and iOS app stores, where it will be free for the first two weeks of release, so please download it and leave some constructive feedback and a review.
The app features tutorials on ECG analysis, exercise and ambulatory ECG, cardiac flow and cycles, action potentials and useful formulae for trace analysis. Each section is laid out in an easy to follow format, with colourful diagrams and both real and illustrated ECG traces.
Heart rate and QTc calculators are included to aid analysis without leaving the app, and also access to the website blog, so you need never miss an update.
This slideshow requires JavaScript.
I hate advertisements in apps, so in order to keep TSP mobile ad-free, I will charge £1 to download it after these introductory 14 days are over. In an ideal scenario, I would keep it completely free, but it has been, and continues to be, a rather expensive endeavour from both a chronological and economical standpoint especially for my shallow, student pockets, so I hope you understand why I have decided to charge.
Stay tuned to TSP via site, Twitter or email for a release date. It’s very soon!
On the 24th of September, the BBC reported the story Nina Adamowicz. Nina, a 72 year old lady with an Implantable Pulse Generator (IPG) who, after having the device for almost 20 years, has requested it be switched off.
After suffering a minor infarct, Adamowicz had said that her continued deteriorating health became too much to bear, said she felt like she was waiting in line to be executed, so she requested her device be switched off. She is reported as stating “It isn’t about ‘I want to die’; I’m dying”.
Her case was referred to her local trust’s ethics committee, who, after careful deliberation decided to proceed in line with the wishes of Mrs Adamowicz.
Before passing away on the same night that her device was switched off, Nina Adamowicz stated that she believed she had the right to decide whether or not she wanted the IPG on or off, and stood by her decision.
This case is thought to be the first of its kind in the UK, but Chicago device specialist Dr Westby Fisher professes to doing this exact thing on a dozen separate occasions. Westby considers the ceased action of an implantable device to removing a feeding tube, or switching off a ventilator.
In particular, in a piece for massdevice.com, Fisher tells of a patient who refused dialysis, saying he’d rather let nature take its course. The patient, who also had an IPG, requested that this was switched off, so Westby agreed, and the next day switched off tachyarrhythmia detection on the device. Fisher says that he feels that both he and his patient did the right thing, together.
I for one, am confused as to the ethical pathway involved in coming to both this decision, and that of the ethics committee associated with Nina Adamowicz.. Assisted suicide is complex, but with respect to these scenarios, is defined as the intentional encouragement or assistance to a patient in ending their own life and it is still illegal under the 1961 Suicide Act of UK law . A medic who administers an overdose of muscle relaxants to a patient whose condition is diagnosed as being terminal, even at the behest of that patient, would be punishable by UK law with manslaughter or murder and potentially serve the maximum terms associated with each.
Why then, is hitting the off switch on a pacemaker not considered to be comparable to the example given previously? Patients with implantable devices often have them to combat life-threatening arrhythmias, so in turning them off, this can effectively issue a death sentence to that patient. I’m not arguing for or against any form of assisted death; I neither understand its intricacies or feel it is my place to denounce or advocate something with which I have had precisely zero experience, I’m simply confused as to why an immediate form of assisted dying is outlawed, and something so similar (on the surface at least), is not. Adamowicz’ clinician has said that other professionals are split in their opinion on his decision, with some feeling it to be “uncomfortably close to euthanasia”.
Is it fair to patients with terminal diagnoses that are forced to travel to countries such as Switzerland, wherein some forms of euthanasia are legal, simply because they do not have an IPG? Does the severity of the condition have any part to play? How similar do individual cases have to be so as to render one illegal and another not so? I have a feeling that this case will spark long debate throughout the medical and legal professions in the UK, and will follow its progress closely.
Like it or loathe it, social media is pretty much inescapable. It’s used by your family, friends, and increasingly by institutions and corporate entities to connect and share ideas, market and promote. Statista puts worldwide social media usage at 2.22 billion people, so it’s no surprise that it has been utilised, and continues to be, to the extent to which we are now accustomed.
It’s been proved that it’s possible to connect with all kinds of people using social platforms, so why should the resource fall solely into the hands of multi-million dollar companies like Coca-Cola and McDonalds, for whom advertising is merely a formality, as oppose to a make-or-break necessity?
Perhaps it needn’t.
Due to the fairly self-regulating nature of some of healthcare’s more specialised areas, the burden falls predominantly on us to showcase innovations and engage with patients, prospective students and fellow professionals. Networking tools like LinkedIn are already being used to connect professionals, even from physiology backgrounds. This platform is relatively self-serving, being a predominantly business to business niche, but according to current statistics it has seen a rise in use to over 60 million views per month in 2016, so is undeniably a great tool to use for quick networking with other like-minded individuals.
Of course, social media can be used to network with everyone, not just our own, so, in the same way that we utilise more than one test to make a diagnosis, we should be using the whole spectrum of tools in this instance, shouldn’t we? Facebook (1.6 billion users worldwide) and Twitter (325 million) usage polls would suggest that users are logging on for a surprisingly narrow selection of reasons. 68% (Twitter) and 65% (Facebook) of users state that they log on to keep abreast of the latest news relevant to themselves, and 63% and 48% of Twitter and Facebook users respectively, use the platforms to receive information relevant to their personal interests. These present huge, potentially untapped resources for healthcare professionals, that can be used to promote transparency and trust, gain feedback and keep colleagues and patients informed.
I’ve mentioned before, the relatively unknown nature of physiology as a profession, so I think that taking hold of the opportunities available on Twitter, and other forms of social media could be something that could benefit physiological science. One of my favourite online healthcare personalities is Mr Olivier Branford, a plastic surgeon in London. He advocates education as a resource that should be available to all, and public engagement as a high priority. Olivier has over 62.1k followers and uses Twitter to provide news relevant to his specialism, and to wider healthcare in general. I conversed with him about the use of social media as a free platform to provide evidence, studies, inspiration and information to students, prospective students and patients everywhere, and we both agreed that it was the perfect resource to utilise. We aren’t alone, however; Olivier ran a telling informal poll, the results of which I have displayed below, enquiring as to what other users believed was the best way for plastic surgeons to use social media, and I feel that the words “plastic surgeon” can be substituted for any within the health service with a similar outcome. As you can no doubt see; despite the unscientific nature of the evidence, the percentages speak for themselves.
Whilst it would be incorrect to state that healthcare organisations have no presence on social media, they don’t dominate in the same way that more commercial entities do, at least not in the UK. That doesn’t necessarily mean that it is a lost cause, however. Mr Branford has provided a personal touch that corporate entities cannot emulate; his approach of “evidence not opinion” when dealing with healthcare information, is complimented by his willingness to offer an opinion when it’s relevant, on top of the facts. This transparency is refreshing, and, in conjunction with his professional accolades, is surely something that has aided him in gaining over 62.1k people who want to listen to what he has to say. The cardiac physiology profession is notoriously under-staffed, and whilst the numbers of applicants is on the increase, a quick visit to various college forums shows that the ins and outs of the career are still lost on many students (if you can find a discussion at all). The general career pathways and the salaries seem to be known to these confused individuals, but the actual job is what nobody has much of an idea about. How are we to persuade these potential cardiac scientists to sign up if they don’t know what they’ll be doing for the rest of their professional lives? Asking someone to commit their future to a career and saddle themselves with increasing debt when they don’t really have a great deal of information readily available to them is a far cry from the informed consent we strive to gain from our patients. Taking responsibility, and putting some research into one’s own future is obviously something everyone has to get used to, but I’m sure most people remember how overwhelming that was, so the shortage of new staff members must be more complicated than students simply not looking hard enough. Besides which, it SHOULDN’T be so difficult to find this career..! I’ve got a year to go until I qualify, and I’ve met some truly inspiring people whom, if I wasn’t already on my way, I know could easily convince me to start. We find what we do fascinating, so surely some of these young minds will be just as invested if they have the chance to see it for themselves.
The Pew Research Centre provides data that places 16-24 year olds as the most avid users of social media (above), and displays a steady growth of users across all age groups year-on-year since 2005, so with a collective effort, it surely wouldn’t be too difficult to a) entice some of these users who are in the middle of their A-Levels, and unsure of which healthcare profession is for them, and b) come together as a profession in a more open and approachable manner to showcase our science and how much of an impact we have on medical diagnostics.
Olivier Branford is a plastic surgeon and associate editor of PRS Global Open journal, and can be found on Twitter under his eponymous handle @OlivierBranford.
Social media statistics obtained from The Pew Research Centre, Statista & Visually
Recently, in a Holter clinic, I dealt with an 8 year old patient who was on the road to recovery after a diagnosis of congenital defect, Tetralogy of Fallot. As a result, I got hold of the most interesting ECG I have recorded to date.
Background
ToF is a rare congential defect affecting the heart, that results in an insufficiency of oxygenated blood leaving the heart through the systemic circulation. Thus, it is considered a cyanotic disorder.
The disorder affects roughly 5 in 10,000 infants, and has an equal gender distribution.
Generally, four pathologies comprise ToF. Whilst all four are not always present, three can consistently be found. ToF is a progressive disorder, in that each pathology gives rise to the others.
Hole in septum, due to malformation, causing oxygenated and deoxygenated blood to mix within cardiac structure
Overriding Aorta
Aorta is placed over VSD, transporting blood with low O2 content to wider systemic circulation
Cyanotic episodes require immediate correction, before surgical intervention.
High flow O2 administration
Physical positioning
Knees to chest
Parent cradling the child will illicit this effect naturally
NaCl fluid bolus
Vasopressor therapy
Increases systemic vascular resistance, shunting blood through pulmonary system.
Continuous ECG and SpO2 monitoring
Surgical intervention usually repairs the VSD and addresses pulmonary pathology, often at the same time.
Prognosis for ToF patients is generally very good.
Overall outcome improved since surgical treatment has improved
Survival of surgery is currently 95-99%
36 year post-surgical survival is currently 96%
Patients who undergo surgical treatment are at greater lifelong risk of ventricular arrhythmia
Complications can arise as a result of a transannular patch repair, specifically;
RV dysfunction
Heart block (risk of HB has dropped to around 1%, in recent studies)
Heart failure
Recurrent or residual VSD
Hx:
8 y/o
Previous diagnosis of ToF
VSD
PV Stenosis
Mild RVH
Treatment:
Transannular patch repair
PV Replacement
Medication:
Daily:
Atenolol
Aspirin
This patient was having a 24hr Holter recording to assess cardiac recovery after their most recent procedure; the PV replacement. Physical examination showed a RVOT murmur, whilst echocadiography displayed a mild RVH and PV regurgitation. Left heart functionality has been classed as excellent.
Previous ambulatory study has shown no arrhythmic action, save for that considered normal in a child of this age. No previous ECG recordings were available.
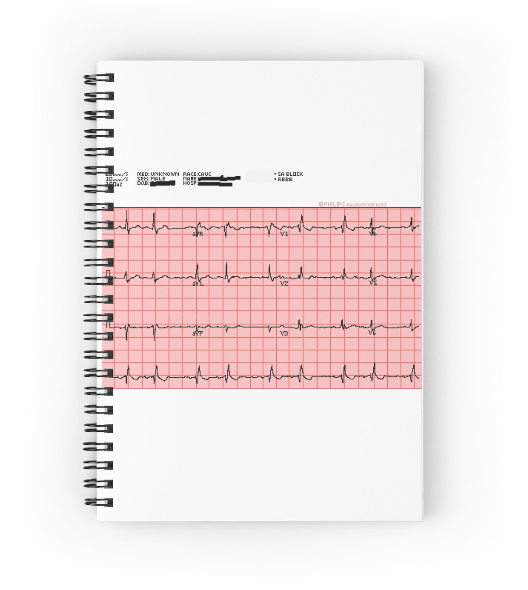
Upon monitor removal, a 12-Lead ECG was performed, the resulting trace was as follows:
Ambulatory analysis relating to the most recent study did not differ greatly from previous monitoring, showing occasional sinus arrhythmia and bradycardia, five non-conducted P waves were found, and two of these gave rise to periods of sinus bradycardia. All other instances were gradual onset/offset.
Nocturnal bradycardia reached rates as low as 34bpm.
What does everyone think of this ECG and brief ambulatory report? Let us know by leaving a comment below!
Studying ECG can be one hell of a mountain to climb, especially when you’re at the novice level of cardiac education. Due to how vital it is, it’s imperative that you can not only make the distinction between Mobitz II AV Block and sinus arrhythmia, but also understand the intricacies of the cardiac conduction behind them, and all of the other rhythm abnormalities. Learning these things like the back of your hand is one thing, but combining all that knowledge is, at times, overwhelming. So after 12 months of scouring the internet, trying to find a decent cardiac anatomy and 12-lead ECG simulation tool, I was over the moon to stumble upon Epicardio Simulation; a cardiac electrophysiology tutorial application, developed by Epicardio ltd.
The program is available in 3 main forms; Epicardio ECG, ECG and Pacing, and 3-day trial. As I don’t have £149 kicking around (the price of the basic ECGcentric offering), I can’t review the full version and all of its features, but the 3 day trial version (which is £0), is well within my price range. Thus, I shall only be commenting on the features with which I have been able to sample.
Thankfully, the collection of features available to trial version users is still extensive, so I have lots to cover, and perhaps I’ll spring for the full version when funds allow. The question is: does the trial impress enough to warrant the large expense? Let’s investigate further:
Almost as soon as you open Epicardio, the vibrant display hits you; a large, anatomically accurate heart fills most of the screen as colourful depolarisation waves travel across the atria, and down through the ventricles. The live single lead ECG tracks with concordance, and the right hand menu buttons are nicely presented and clearly display exactly what they do.
Depolarisation mechanics can be viewed through the heart as a whole, or each section on its own. Atria, ventricles, bundle branches and coronaries, can all be viewed independently whilst depolarisation occurs, so it’s possible to learn how the various components of the cardiac system operate during each cycle.
Further structural overlays can be added, in the form of the vena cava, thoracic cage and a translucent torso, further adding to the ability to understand the heart’s positioning in humans.
The electrical readout on the lower region of the screen comes with the option of cycling through all 12 leads on the standard ECG, individually, but as well the real time single lead ECG, users can also activate a live 12-lead, which again updates in real time with each cardiac cycle. This mode itself allows for different viewing styles, including the layout presented on most standard ECG printouts, which is perfect for students. It also features all the subtle morphology differences and minor, unavoidable muscle tremors that one would find on a real ECG recording. Calipers are a welcome feature, too, and they work well in Epicardio, allowing for measurements that students will definitely have to become proficient in throughout training.
Further customisation options are numerous; the colours of the depolarisation waves are changeable, as is the colour of the backdrop. Rather than simply offering pre-set rhythms, Epicardio allows you to manually alter heart rate, and, possibly more importantly, AV delay, so it’s possible to visibly alter the depolarisation wave on the beating heart in the centre of the screen, and see the live trace display a prolonged PR interval.
A most welcome feature is the electrode view option. A click on this button brings up a moving image of the heart within the thorax, and the standard precordial electrode sites. These electrodes can be moved anywhere and the real-time result displayed on the recorded trace, so it’s rather nice to be able to explore the difference in the voltage/time graph that occurs with electrode misplacement.
A defibrillator option allows you to shock the heart, although this was of limited use to me, as I did not have access to the fibrillatory rhythms that come with the paid version, but the artificial pacemaker below it allows the user to alter pacing pulses and observe the changes on the ECG.
My issues with Epicardio range from those that exist simply because the version I tried is restricted, to those that are nought but minor niggles, so I shall focus on those minor niggles, as oppose to content I simply have not paid to access.
The ECG trace, whilst being incredibly customisable, would feel much more authentic if it were set against a proportional image of standard ECG paper; being able to view the trace against the background most students will see throughout studies would be a great primer in the early days of study, and considering the trace speed is adjustable, I was disappointed it wasn’t a feature.
The option buttons look lovely, offer genuine function and, once you’ve been through the tutorial and played around with them, make perfect sense. It would perhaps be helpful if a brief explanation appeared when the mouse pointer was placed over each one, however, as it was a struggle remembering what the more vague options actually did, especially for the first few hours of using the program.
However, as I stated, these are only minor gripes. Epicardio is a wonderful and genuinely fun bit of software to use. I’ve got a feel for how beneficial having this in the beginning of my studies would have been. The layout, options, functionality and simplicity of using Epicardio are all near-perfect, so I can’t wait to get a hold of the full version, complete with pacemaker-specific options. If you have a spare weekend, then follow the link at the top of the page, and download the free trial. If you have a spare £149/£215, then follow the same link and download the full version, as if it’s provides even 50% more features than the demo, I can be certain it’s worth it.
I’ve added some new work to the online store. Head over there and you can find work inspired by Torsades de Pointes, an anatomical representation of a pacemaker in situ and an illustrated (and truncated) chronology of pacemakers (I’ve been doing some pacing).
As with those already up, these designs are available on mugs, books and smartphone cases, as well as clothing.
Remember, every penny made via sales goes straight back into this website.
After creating so many illustrations for the various study pages I have added (and a few future ones), I thought it might be nice to put them to more use.
Many of the original images you see on this website can now be worn, written in, or used to hold beverages when you’re on placement! A selection of the items available are on display here, but do go and check out the store to have a look at everything on offer. They’re all of a high-quality and available in a variety of styles, too, so I hope you find something you like.
I’ll keep adding new designs, so be sure to check back often, and every penny made through sales will go towards furthering this website.
BMJ Best Practice is an app that aims to aid diagnosis and guide the practitioner through the treatment process of a number of pathologies. Guidelines on examinations, tests and medications are provided across 977 topics. These are not all available initially; some conditions are presented as a free sample, whilst the rest must be purchased either in one go (£59.99), or by categories such as Critical Care and Emergency Medicine (£15.99), and Cardiovascular Disorders, Vascular and Cardiothoracic Surgery (£7.99). Institutional access is available, so if your trust/ university subscribes to the service, you can access all of the content for free.
These are the good things BMJBP does. Unfortunately, it does a great deal worse when it comes to every other aspect of its content and execution.
Whilst the level of content is very good, straightforward and to the point, it’s unlikely that you’ll actually get to see any of it, as the sample pages don’t always load, and when they do, they don’t save. Frequently, I left the app to take a call, and returned to it to find it had rebooted. In addition, whilst the developer’s ability to extract the subscription fee for paid content suffers no problems, their ability to supply said content is non-existent. I purchased the “Cardiovascular Disorders…” category for £7.99, and was told by the “My Topics” section of the app, that I didn’t own any of the documents, yet was told by the “Subscribe” page, that I did..! Either way, I couldn’t (and still can’t) view any of the content I have paid for.
I sent an email over to the BMJ customer service department, and was politely informed that subscriptions were handled by Google, and there was nothing that BMJ could themselves do. As it turns out, subscribed content is entirely the responsibility of the BMJ, so when I pointed this out, and asked for a refund, I was met with a wall of silence that is currently ongoing.
Although it may be tempting to download this app, I strongly recommend that you do not; the content isn’t there, the app itself is buggy and the developer’s desire to help with problems is as present as the paid topics, in that both have yet to materialise. Judging by the user reviews left on Google Play, I am not the only user to have faced any of these problems, so it’s not as though the devs are unaware.
This app doesn’t do enough, regarding functionality, to warrant being this unfinished. It genuinely frightens me to think that someone was paid a wage to develop this, and even more frightening, is that the BMJ are charging for content, despite the numerous complaints of bugs and such. The app lists its last update as 2015, but lord knows what it addressed, or how much worse it was before, if this is considered sufficient.
This, dear reader, is how NOT to make a mobile app.
I had the rather marvellous opportunity today; spending a day in cardiac theatres and, under the guidance and tutelage of two cardiac surgeons and an anaesthetist, learning the processes and methodologies behind CABG and MV repair.
I arrived at the Bristol Royal Infirmary surgical centre at 7:45am and was quickly changed into some scrubs and inducted into the OR’s team: three surgeons, two anaesthetists, one perfusionist and a selection of nurses both scrub, and regular. It was clear to me that each of these individuals knew one another well, just by the way they talked to each other; everyone seemed at ease with the rest of their colleagues. It turns out, I was right. Many of them knew each other from other hospitals, university or simply having been mentored by each other during training. This camaraderie bled into the surgery, as each team member knew not only their role, but that of the others, also, so equipment was passed over or set up without being requested, making for a seamless procedure.
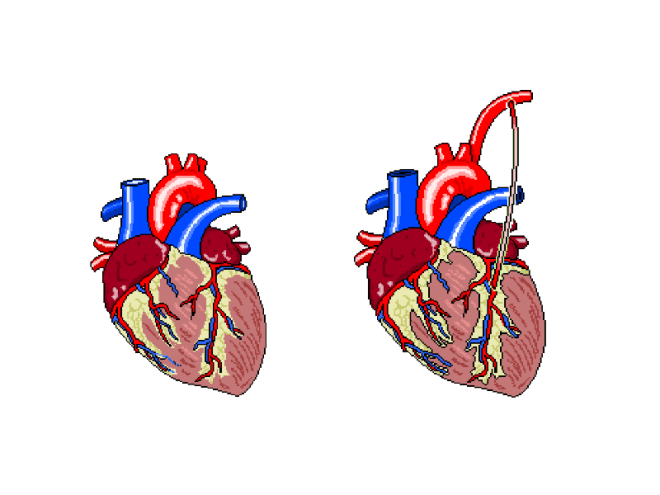
The patient was, until the last year or so, a very fit and active 79y/o, who had suffered from AF for at least 10 years, and had developed a stenosed left anterior descending coronary artery as a result. In addition, echo had shown a severe mitral regurgitation due to valvular prolapse. The procedure would attempt to bypass the LAD using the left internal mammary artery (LIMA), as shown below.
Figure 1: The left internal mammary artery (shown in situ on the right) is relocated from the chest wall to bypass the stenosed section of the LAD.
The plan was to perform the bypass graft, and then set about repairing the damaged mitral valve.
After the patient’s ID and contraindicators had been checked, the anaethetists set about carefully monitoring their respiratory and cardiovascular function as the GA took effect. The ECG, arterial and venous pressure traces were available on lots of screens around the rooms, as whilst they must be monitored all of the time, it becomes particularly important to keep an eye on the given values as the heart is both stopped and re-started.
Interestingly, I noticed a pattern in conversation with each patient throughout the day, as the anaesthetic was administered. The patient was asked to think of their favourite place and the team then asked where that place was. Each time, this was met with silence, but just to make sure, the patient was always asked if they were warm enough. When no answer was forthcoming, they were wheeled into the theatre room proper.
Not everyone on the team was scrubbed up and sterilised, as obviously some would not be required to touch the patient, and others would be required to fetch replacement equipment should it be needed. This created a “sterile field” around the operating table, so only sterile members of staff were permitted within it.
After 1 hour and a whole heap of sterile gowns and drapes were applied over the patient, with only a small window showing the surgical site, the operation began.
Step 1 required access to the thoracic cavity. In case of blood splatter, masks fitted with facial protection were supplied to myself and the other team members who would be in the direct vicinity of the patient when the chest was opened.
An incision was made as illustrated below. This is known as a median sternotomy, and extends from the sternal notch to the xyphoid process. In order to progress past the sternum, an oscillating saw is used to cut throught it. There is a surprising amount of finesse involved in this stage, despite how much pressure is required and as a result, how brutal it appears.
The incision is deepened and cauterised until it travels through the pericardium, so as to allow access to the heart and, after the bleeding vessels around the wound are cauterised, a finochietto retractor is used to hold the sternum open. During this time, the LIMA is found and carefully removed from the chest wall. It is then held in an accessible place with forceps, to be used later.
Lung and cardiac function is transfered to a cardiopulmonary bypass machine, which allows both the heart and lungs to be stopped/emptied, allowing even greater access to the heart due to the lack of lung obstruction, and intricate work to be perfomed whilst the heart is not beating.
The cardiopulmonary bypass apparatus purifies the blood that passes through it from the patient via cannulas placed in the heart and pumps it back, thereby doing the work of the heart and lungs. The heart is fed nutrients at the same time, so as to keep it healthy for the extended period of inactivity. This method of on-pump surgery is known to be incredibly safe- between 1 and 2% of high risk patients will suffer adverse effects as a result of the treatment, and surgical teams are well versed in assessing this via risk factors.
Once the LAD has been correctly identified, an incision is made, creating an opening that roughly matches the size of the end of the LIMA, and the two are stitched together using sutures made of polypropylene,which are no thicker than a human hair, yet can withstand the pressure that would be required to rupture a healthy vessel. To test the suture site, blood is passed through the vessel, and in the event of any gaps in the connection, this blood will be seen outside of the join, which can then be further secured as necessary.
The process, whilst quick to document, was a long one, as each step of the technique was scrutinised carefully before considered complete. In addition, each stitch required at least two people directly, to exact it; one to add the suture, and the rest to support the structures surrounding it.
The second stage of this case was the mitral valve repair, which was in itself a multi-stepped procedure. It is possible to repair a damaged mitral valve using less invasive, keyhole methods, but due to the need for a bypass graft, this wasn’t an option this time.
After gaining access to the valve itself, via an incision in the left atrium, the condition of the valve leaflets is assessed. This particular patient’s posterior leaflet had a prolapsing middle scallop, which meant that the below procedure was necessary to repair it.
The process off attaching the ring was a long one, involving a lot of organisation and intricate knotting. The sutures are applied to both the ring and the valve, the latter is then gently pushed down the threads and into place. These suture strings are then tied off and cut.
Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.
When performing the annuloplasty removed the surplus anterior leaflet, it took with it a tendineae chordeae, so in order to stabilise it further, an artificial heart string (made of Gore-Tex) was attached to the leaflet and papillary muscle.
A final transesophageal echo was performed, to assess the level of air still present in the heart, and to then assess the function of the repaired mitral valve, and after all of this was successfully accomplished, the long task to gently remove all of the cannulas that were used to bypass the cardiopulmonary system were begun to be removed. Each chamber was sutured in sequence, and the corresponding section of the perfusion apparatus turned off. All of this time, the anaesthetist monitored the patient’s drug infusions and every member of the team monitored pressure and ECG traces. This was still going on whilst the SpR set about cauterising vessels and wiring the sternum before pulling it back together. None of this section of the procedure involved any real finesse; pulling the wires taut so as to close the chest cavity is a test of strength. Each pull caused the patient to move for the first time since coming into the theatre, so I guess that was why it was the only section of the surgery that almost made me wince (something the theatre lead noticed and laughed about). Once it was done, the multiple layers of sutures were applied to seal the surface wound and the patient was taken to recovery.
In all honesty, the most difficult part for me, was in standing for so long. This was echoed by the surgeons, who said that they always felt backed up by their colleagues, so they felt confident that the procedure itself would go well, but standing, often in an unnatural position for so six hours at a time played havoc with their backs and legs. The anaesthetists, being required fully at the beginning and the end of the surgery, spent a great deal of time sat waiting, save for occasionally changing an infusion as and when required. The people working solidly were the surgeons and the scrub nurse, but even the surgeons swapped roles, observed one another without participating, and even took breaks periodically. None of this diminishes any one role, however; each member of the team was required, be it constantly or otherwise, and when one was needed, it took a single word for everyone in the room to know what was required, and by whom. Despite the procedure itself being amazing, it was the mechanical and seamless nature of the professionals in the room that was the most astounding part of the day.






































 Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.
Once this has been completed, the valve integrity and functionality was tested by flushing water through the heart. In this case, the valve was still slightly prolapsing, as the water flushed through the valve in an unwanted quantity. The entire process, then, was considered from the beginning, and the valve only said to be repaired, when the regurgitation seen through the valve was minimal.